

NT-proBNP and Its Correlation with In-Hospital Mortality in the Very Elderly without an Admission Diagnosis of Heart Failure
- PMID: 27077910
- PMCID: PMC4831737
- DOI: 10.1371/journal.pone.0153759
NT-proBNP and Its Correlation with In-Hospital Mortality in the Very Elderly without an Admission Diagnosis of Heart Failure
Abstract
Background: The diagnosis of heart failure (HF) is often difficult and underestimated in very elderly comorbid patients, especially when an echocardiographic evaluation is not available or feasible.
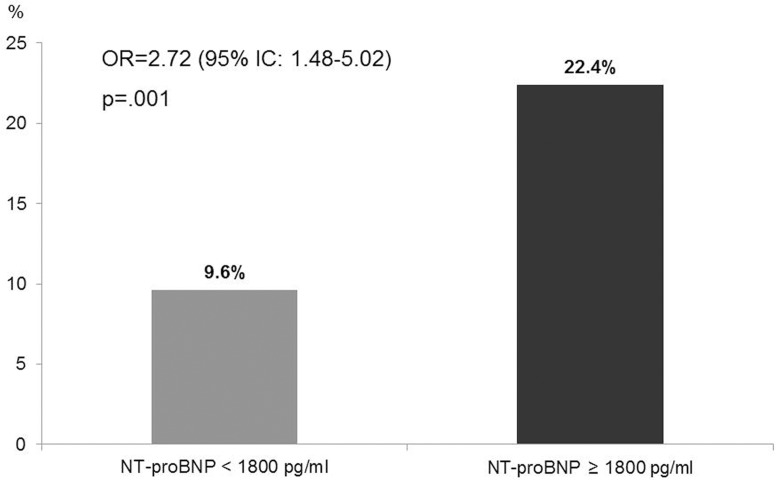
Aim: to evaluate NT-proBNP values and their correlation with in-hospital mortality in a population of very elderly hospitalized for medical conditions other than HF.
Methods: We performed a prospective observational study on 403 very elderly admitted to an Internal Medicine and Geriatrics Department. Exclusion criterion was an admission diagnosis of HF. Patients with at least one symptom or sign compatible with HF were tested for NT-proBNP. NT-proBNP values < 300 pg/ml were considered as an age-independent exclusion criterion for HF (high negative predictive value), while NT-proBNP values ≥ 1800 pg/ml were considered as a diagnostic criterion. Main comorbidities and laboratory parameters were considered to adjust regression analyses between NT-proBNP and in-hospital mortality.
Results: NT-proBNP values ≥ 1800 pg/ml were present in 61.0% of patients and 32.8% of patients laid between 300 ≤ NT-proBNP < 1800 pg/ml values. NT-proBNP values were associated with the main indices of disease severity/organ failure considered such as reduced eGFR, reduced albumin and elevated CRP. NT-proBNP values ≥ 1800 pg/ml and ln(NT-proBNP) values were significantly associated with in-hospital mortality independently from the main comorbidities and lab parameters considered. The patients, who were already taking ACE inhibitors/Angiotensin Receptor Blockers before admission, showed lower in-hospital mortality.
Conclusions: Testing for NT-proBNP should be strongly recommended in the hospitalized very elderly, because of the very high prevalence of underlying HF and its impact on in-hospital mortality, to identify an underlying cardiac involvement that requires appropriate treatment.
Conflict of interest statement
Figures
References
-
- McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Böhm M, Dickstein K, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Eur Heart J. 2012; 33(14): 1787–847 10.1093/eurheartj/ehs104 - DOI - PubMed
-
- Schocken DD, Benjamin EJ, Fonarow GC, Krumholz HM, Levy D, Mensah GA, et al. Prevention of heart failure: a scientific statement from the American Heart Association Councils on Epidemiology and Prevention, Clinical Cardiology, Cardiovascular Nursing, and High Blood Pressure Research; Quality of Care and Outcomes Research Interdisciplinary Working Group; and Functional Genomics and Translational Biology Interdisciplinary Working Group. Circulation 2008; 117(19): 2544–65 10.1161/CIRCULATIONAHA.107.188965 - DOI - PubMed
-
- Database of the Italian Ministry of Health. Statistics of hospital admissions. Available at: http://www.salute.gov.it/ricoveriOspedalieri/ric_informazioni/interrogad...
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
