

Glaucoma Surgery Calculator: Limited Additive Effect of Phacoemulsification on Intraocular Pressure in Ab Interno Trabeculectomy
- PMID: 27077914
- PMCID: PMC4831696
- DOI: 10.1371/journal.pone.0153585
Glaucoma Surgery Calculator: Limited Additive Effect of Phacoemulsification on Intraocular Pressure in Ab Interno Trabeculectomy
Abstract
Purpose: To compare intraocular pressure (IOP) reduction and to develop a predictive surgery calculator based on the results between trabectome-mediated ab interno trabeculectomy in pseudophakic patients versus phacoemulsification combined with trabectome-mediated ab interno trabeculectomy in phakic patients.
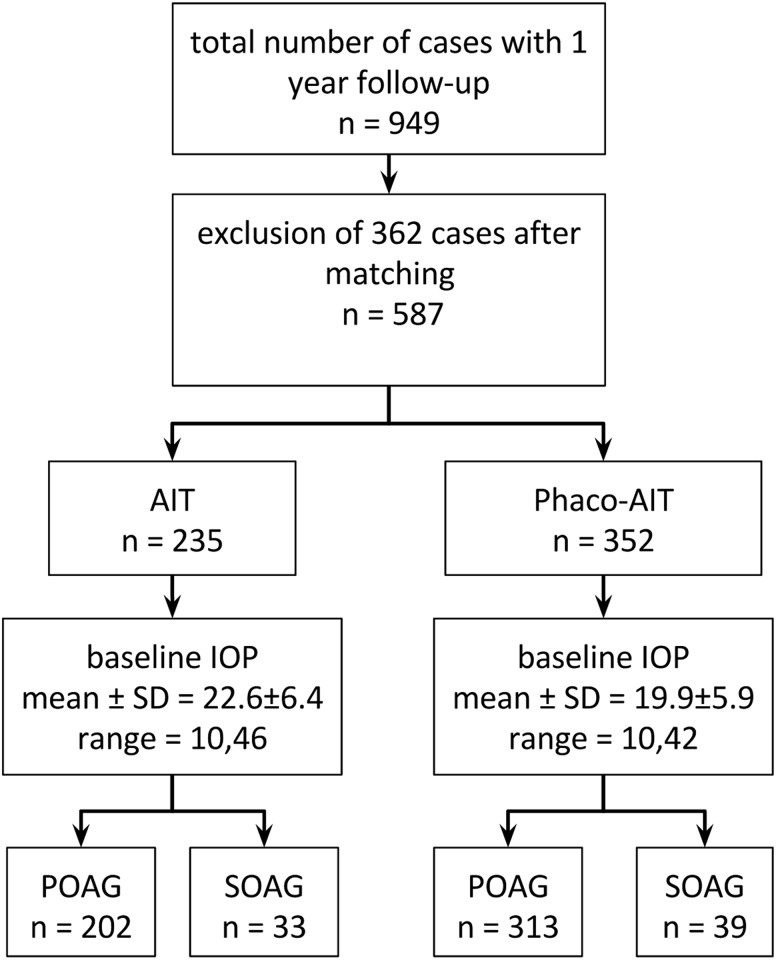
Methods: This observational surgical cohort study analyzed pseudophakic patients who received trabectome-mediated ab interno trabeculectomy (AIT) or phacoemulsification combined with AIT (phaco-AIT). Follow up for less than 12 months or neovascular glaucoma led to exclusion. Missing data was imputed by generating 5 similar but non-identical datasets. Groups were matched using Coarsened Exact Matching based on age, gender, type of glaucoma, race, preoperative number of glaucoma medications and baseline intraocular pressure (IOP). Linear regression was used to examine the outcome measures consisting of IOP and medications.
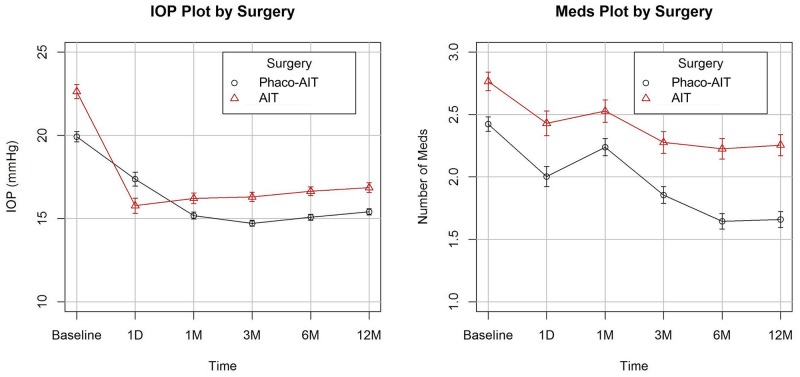
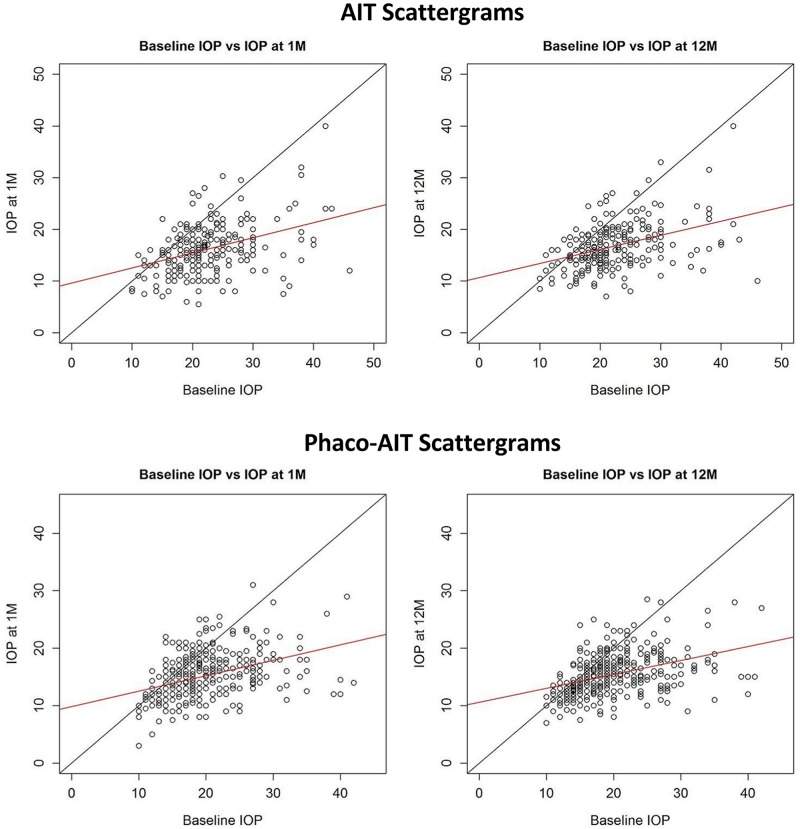
Results: Of 949 cases, 587 were included consisting of 235 AIT and 352 phaco-AIT. Baseline IOP between groups was statistically significant (p≤0.01) in linear regression models and was minimized after Coarsened Exact Matching. An increment of 1 mmHg in baseline IOP was associated with a 0.73±0.03 mmHg IOP reduction. Phaco-AIT had an IOP reduction that was only 0.73±0.32 mmHg greater than that of AIT. The resulting calculator to determine IOP reduction consisted of the formula -13.54+0.73 × (phacoemulsification yes:1, no:0) + 0.73 × (baseline IOP) + 0.59 × (secondary open angle glaucoma yes:1, no:0) + 0.03 × (age) + 0.09 × (medications).
Conclusions: This predictive calculator for minimally invasive glaucoma surgery can assist clinical decision making. Only a small additional IOP reduction was observed when phacoemulsification was added to AIT. Patients with a higher baseline IOP had a greater IOP reduction.
Conflict of interest statement
Figures
References
-
- Shingleton BJ, Pasternack JJ, Hung JW, O’Donoghue MW. Three and five year changes in intraocular pressures after clear corneal phacoemulsification in open angle glaucoma patients, glaucoma suspects, and normal patients. J Glaucoma. 2006;15: 494–498. - PubMed
-
- Iordanous Y, Kent JS, Hutnik CML, Malvankar-Mehta MS. Projected cost comparison of Trabectome, iStent, and endoscopic cyclophotocoagulation versus glaucoma medication in the Ontario Health Insurance Plan. J Glaucoma. 2014;23: e112–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
