

Airway Microbiota in Severe Asthma and Relationship to Asthma Severity and Phenotypes
- PMID: 27078029
- PMCID: PMC4831690
- DOI: 10.1371/journal.pone.0152724
Airway Microbiota in Severe Asthma and Relationship to Asthma Severity and Phenotypes
Abstract
Background: The lower airways harbor a community of bacterial species which is altered in asthma.
Objectives: We examined whether the lower airway microbiota were related to measures of asthma severity.
Methods: We prospectively recruited 26 severe asthma, 18 non-severe asthma and 12 healthy subjects. DNA was extracted from induced sputum and PCR amplification of the V3-V5 region of bacterial 16S rRNA gene was performed.
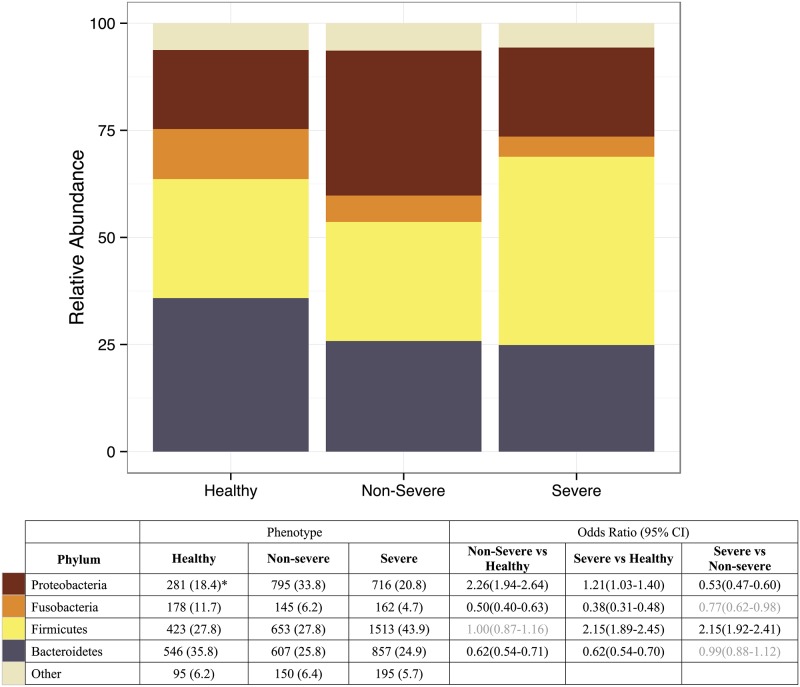
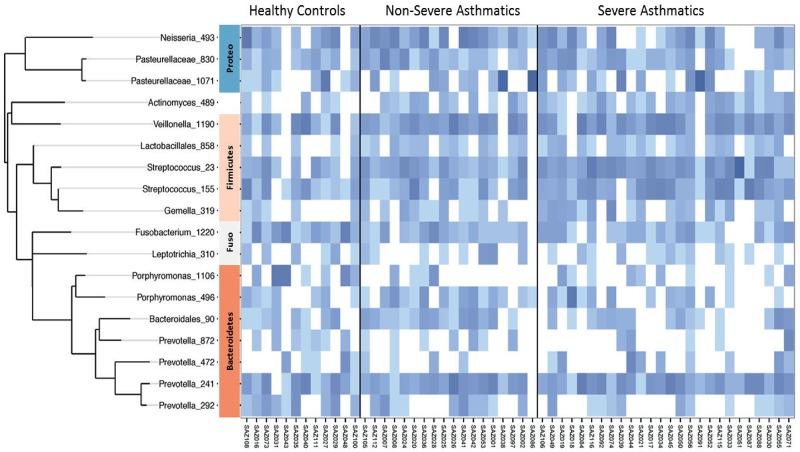
Results: We obtained 138,218 high quality sequences which were rarefied at 133 sequences/sample. Twenty OTUs had sequences ≥1% of total. There were marked differences in the distribution of Phyla between groups (P = 2.8x10-118). Bacteroidetes and Fusobacteria were reduced in non-severe and severe asthmatic groups. Proteobacteria were more common in non-severe asthmatics compared to controls (OR = 2.26; 95% CI = 1.94-2.64) and Firmicutes were increased in severe asthmatics compared to controls (OR = 2.15; 95%CI = 1.89-2.45). Streptococcal OTUs amongst the Firmicutes were associated with recent onset asthma, rhinosinusitis and sputum eosinophilia.
Conclusions: Sputum microbiota in severe asthma differs from healthy controls and non-severe asthmatics, and is characterized by the presence of Streptococcus spp with eosinophilia. Whether these organisms are causative for the pathophysiology of asthma remains to be determined.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
