

Trends in the Burden of Adult Congenital Heart Disease in US Emergency Departments
- PMID: 27079279
- PMCID: PMC6490840
- DOI: 10.1002/clc.22541
Trends in the Burden of Adult Congenital Heart Disease in US Emergency Departments
Abstract
Background: We assessed trends in incidence, in-hospital mortality, and admission among patients with adult congenital heart disease (ACHD) presenting to the emergency department (ED) from 2006 to 2012.
Hypothesis: There is a considerable burden of ACHD in the US EDs.
Methods: We used the 2006-2012 US Nationwide Emergency Department Sample. All ED visits with ACHD were identified using standard International Classification of Diseases, Ninth Edition, Clinical Modification codes.
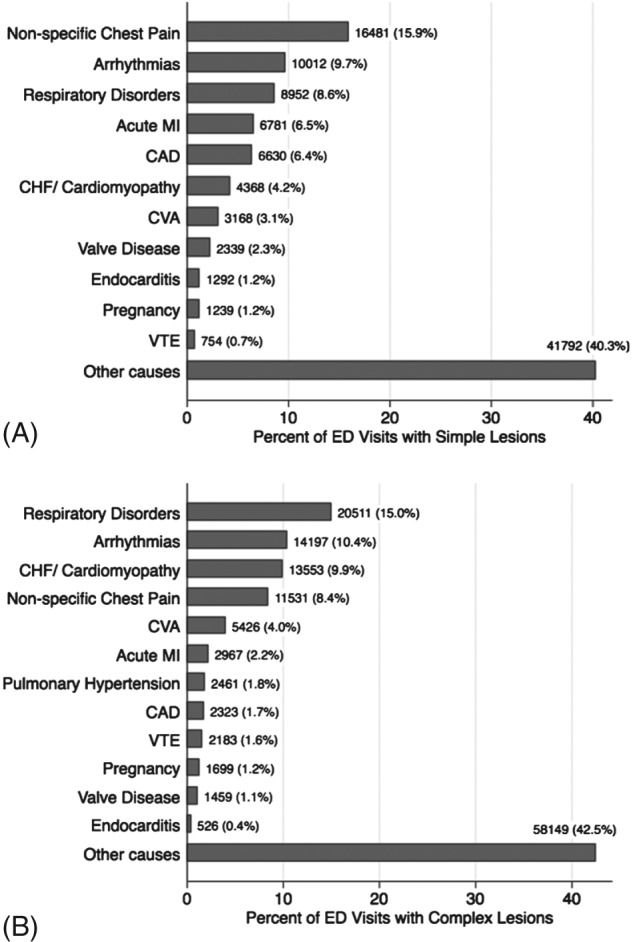
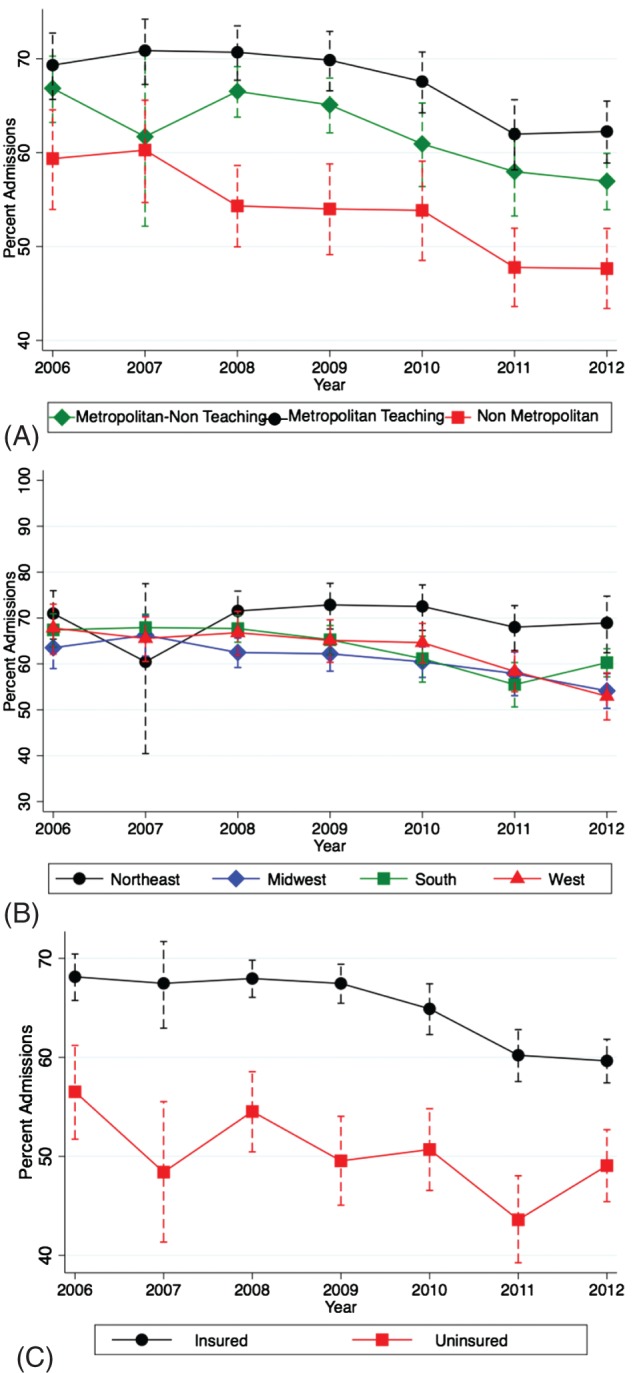
Results: The number of patients presenting to the ED with simple (40.6%) as well as complex (37.6%) ACHD across 2006-2012 increased significantly. Also, there was a considerable increase in prevalence of traditional cardiovascular risk factors among ACHD patients, including hypertension, diabetes, smoking, obesity, and chronic kidney disease. Besides miscellaneous noncardiovascular conditions, nonspecific chest pain (15.9%) and respiratory disorders (15.0%) were the most common reasons for ED visits among patients with simple and complex ACHD, respectively. Although there was a trend toward decrease in admissions across 2006-2012 (Ptrend < 0.001), the proportion of patients with ACHD presenting to ED requiring admission remained substantial (63.4%). Finally, there was significant variation in admission trends across different geographic locations, hospital types, insurance status, and ED volume among ACHD patients presenting to the ED.
Conclusions: There has been a progressive increase in number of ED visits among ACHD patients across 2006-2012 in the United States. Moreover, the cardiovascular risk-factor profile of ACHD patients has changed, adding to complexity in management. Current health care delivery to ACHD patients also shows significant geographical, hospital-based, and insurance status-based disparities.
© 2016 Wiley Periodicals, Inc.
Figures


References
-
- Kellermann AL. Crisis in the emergency department. N Engl J Med. 2006;355:1300–1303. - PubMed
-
- Pitts SR, Pines JM, Handrigan MT, et al. National trends in emergency department occupancy, 2001 to 2008: effect of inpatient admissions versus emergency department practice intensity. Ann Emerg Med. 2012;60:679.e3–686.e3. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
