

Diabetes and Stroke: Epidemiology, Pathophysiology, Pharmaceuticals and Outcomes
- PMID: 27079344
- PMCID: PMC5298897
- DOI: 10.1016/j.amjms.2016.01.011
Diabetes and Stroke: Epidemiology, Pathophysiology, Pharmaceuticals and Outcomes
Abstract
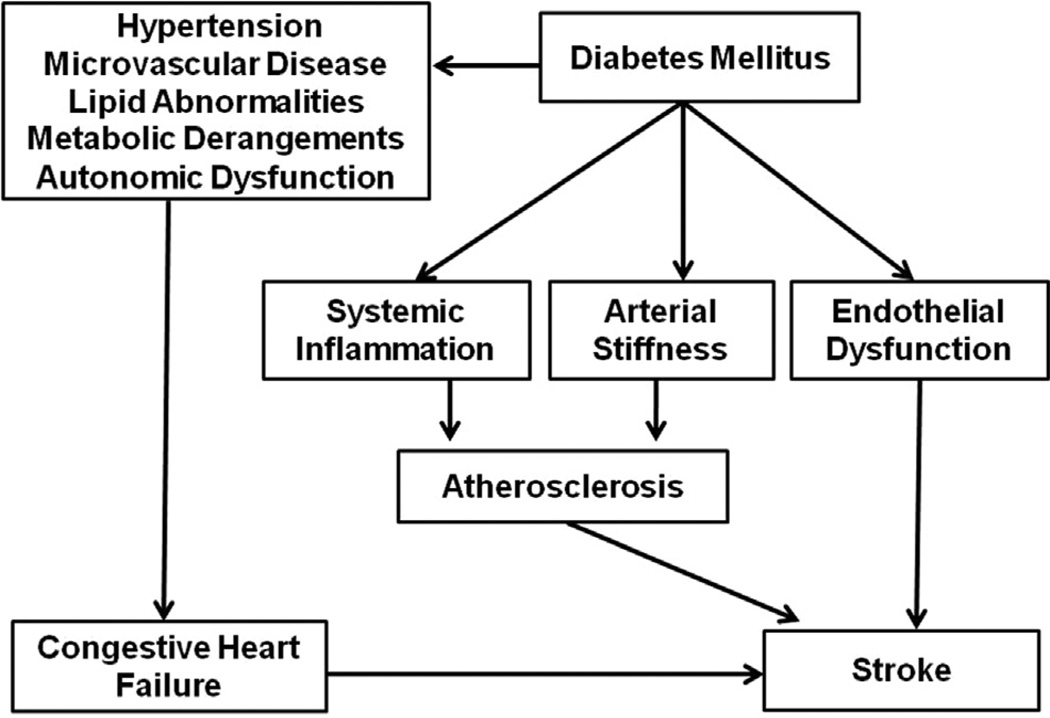
There has been a significant increase in obesity rates worldwide with the corresponding surge in diabetes. Diabetes causes various microvascular and macrovascular changes often culminating in major clinical complications, 1 of which, is stroke. Although gains have been made over the last 2 decades in reducing the burden of stroke, the recent rise in rates of diabetes threatens to reverse these advances. Of the several mechanistic stroke subtypes, individuals with diabetes are especially susceptible to the consequences of cerebral small vessel diseases. Hyperglycemia confers greater risk of stroke occurrence. This increased risk is often seen in individuals with diabetes and is associated with poorer clinical outcomes (including higher mortality), especially following ischemic stroke. Improving stroke outcomes in individuals with diabetes requires prompt and persistent implementation of evidence-based medical therapies as well as adoption of beneficial lifestyle practices.
Keywords: Diabetes; Hyperglycemia; Outcomes; Stroke; Stroke prevention.
Copyright © 2016 Southern Society for Clinical Investigation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Heidenreich PA, Trogdon JG, Khavjou OA, et al. Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation. 2011;123:933–944. - PubMed
-
- Putaala J, Liebkind R, Gordin D, et al. Diabetes mellitus and ischemic stroke in the young: clinical features and long-term prognosis. Neurology. 2011;76:1831–1837. - PubMed
-
- O'Donnell MJ, Xavier D, Liu L, et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control study. Lancet. 2010;376:112–123. - PubMed
-
- Wolf PA, D'Agostino RB, Belanger AJ, et al. Probability of stroke: a risk profile from the Framingham Study. Stroke. 1991;22:312–318. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
