

Randomized, multicenter study: on-demand versus continuous maintenance treatment with esomeprazole in patients with non-erosive gastroesophageal reflux disease
- PMID: 27080034
- PMCID: PMC4831110
- DOI: 10.1186/s12876-016-0448-x
Randomized, multicenter study: on-demand versus continuous maintenance treatment with esomeprazole in patients with non-erosive gastroesophageal reflux disease
Abstract
Background: Most patients with gastroesophageal reflux disease experience symptomatic relapse after stopping acid-suppressive medication. The aim of this study was to compare willingness to continue treatment with esomeprazole on-demand versus continuous maintenance therapy for symptom control in patients with non-erosive reflux disease (NERD) after 6 months.
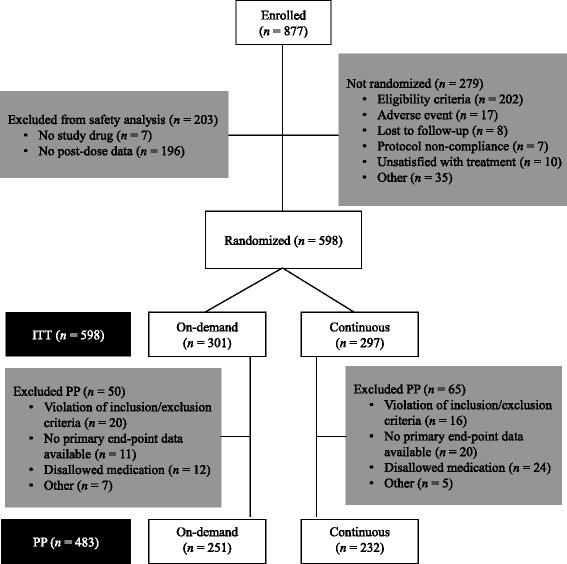
Methods: This multicenter, open-label, randomized, parallel-group study enrolled adults with NERD who were heartburn-free after 4 weeks' treatment with esomeprazole 20 mg daily. Patients received esomeprazole 20 mg daily continuously or on-demand for 6 months. The primary variable was discontinuation due to unsatisfactory treatment. On-demand treatment was considered non-inferior if the upper limit of the one-sided 95 % confidence interval (CI) for the difference between treatments was <10 %.
Results: Of 877 patients enrolled, 598 were randomized to maintenance treatment (continuous: n = 297; on-demand: n = 301). Discontinuation due to unsatisfactory treatment was 6.3 % for on-demand and 9.8 % for continuous treatment (difference -3.5 % [90 % CI: -7.1 %, 0.2 %]). In total, 82.1 and 86.2 % of patients taking on-demand and continuous therapy, respectively, were satisfied with the treatment of heartburn and regurgitation symptoms, a secondary variable (P = NS). Mean study drug consumption was 0.41 and 0.91 tablets/day, respectively. Overall, 5 % of the on-demand group developed reflux esophagitis versus none in the continuous group (P < 0.0001). The Gastrointestinal Symptom Rating Scale Reflux dimension was also improved for continuous versus on-demand treatment. Esomeprazole was well tolerated.
Conclusions: In terms of willingness to continue treatment, on-demand treatment with esomeprazole 20 mg was non-inferior to continuous maintenance treatment and reduced medication usage in patients with NERD who had achieved symptom control with initial esomeprazole treatment.
Trial registration: ClinicalTrials.gov identifier (NCT number): NCT02670642 ; Date of registration: December 2015.
Keywords: Discontinuation; Esomeprazole; Gastroesophageal reflux disease; Heartburn; Non-erosive reflux disease; On-demand.
Figures


References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
