

Use of Coronary Computed Tomographic Angiography to Guide Management of Patients With Coronary Disease
- PMID: 27081014
- PMCID: PMC4829708
- DOI: 10.1016/j.jacc.2016.02.026
Use of Coronary Computed Tomographic Angiography to Guide Management of Patients With Coronary Disease
Abstract
Background: In a prospective, multicenter, randomized controlled trial, 4,146 patients were randomized to receive standard care or standard care plus coronary computed tomography angiography (CCTA).
Objectives: The purpose of this study was to explore the consequences of CCTA-assisted diagnosis on invasive coronary angiography, preventive treatments, and clinical outcomes.
Methods: In post hoc analyses, we assessed changes in invasive coronary angiography, preventive treatments, and clinical outcomes using national electronic health records.
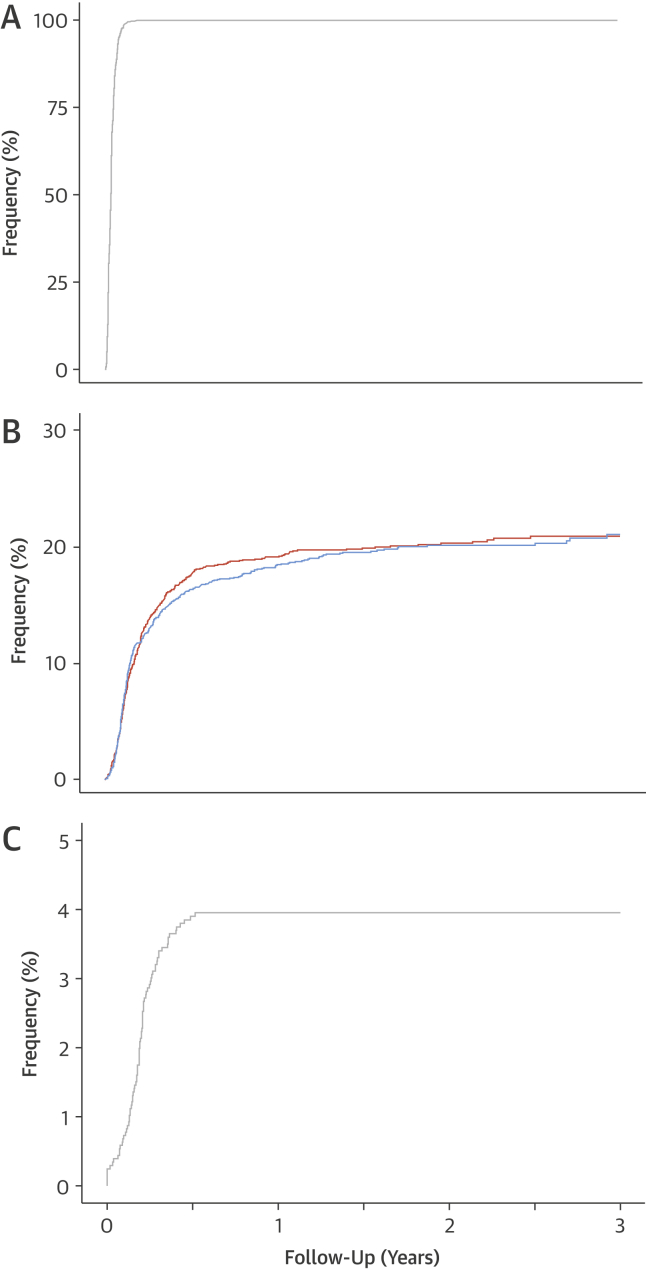
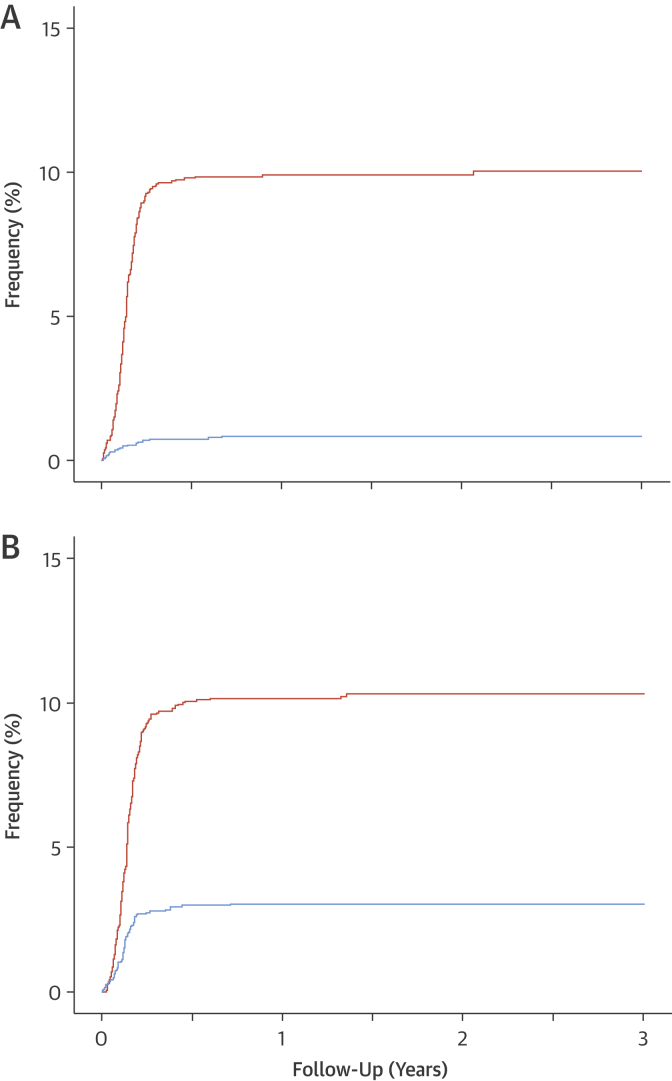
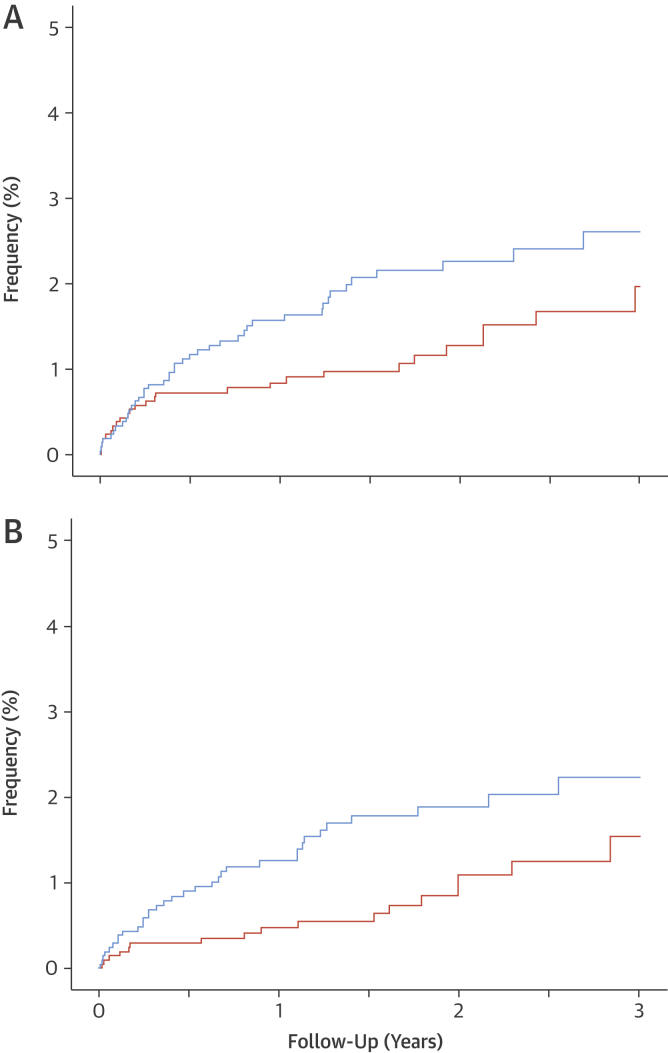
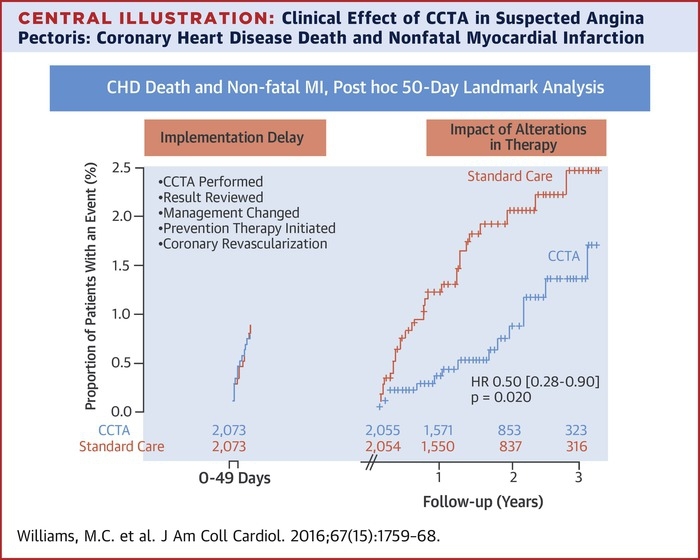
Results: Despite similar overall rates (409 vs. 401; p = 0.451), invasive angiography was less likely to demonstrate normal coronary arteries (20 vs. 56; hazard ratios [HRs]: 0.39 [95% confidence interval (CI): 0.23 to 0.68]; p < 0.001) but more likely to show obstructive coronary artery disease (283 vs. 230; HR: 1.29 [95% CI: 1.08 to 1.55]; p = 0.005) in those allocated to CCTA. More preventive therapies (283 vs. 74; HR: 4.03 [95% CI: 3.12 to 5.20]; p < 0.001) were initiated after CCTA, with each drug commencing at a median of 48 to 52 days after clinic attendance. From the median time for preventive therapy initiation (50 days), fatal and nonfatal myocardial infarction was halved in patients allocated to CCTA compared with those assigned to standard care (17 vs. 34; HR: 0.50 [95% CI: 0.28 to 0.88]; p = 0.020). Cumulative 6-month costs were slightly higher with CCTA: difference $462 (95% CI: $303 to $621).
Conclusions: In patients with suspected angina due to coronary heart disease, CCTA leads to more appropriate use of invasive angiography and alterations in preventive therapies that were associated with a halving of fatal and non-fatal myocardial infarction. (Scottish COmputed Tomography of the HEART Trial [SCOT-HEART]; NCT01149590).
Keywords: angina pectoris; invasive coronary angiography; myocardial infarction; preventive therapy.
Copyright © 2016 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
The Future From the Past: A Chance for Change.J Am Coll Cardiol. 2016 Apr 19;67(15):1769-1771. doi: 10.1016/j.jacc.2016.02.028. J Am Coll Cardiol. 2016. PMID: 27081015 No abstract available.
-
Primum Non Nocere: Old Principle Revisited.J Am Coll Cardiol. 2016 Oct 4;68(14):1602-3. doi: 10.1016/j.jacc.2016.06.066. J Am Coll Cardiol. 2016. PMID: 27687204 No abstract available.
-
Enhanced Preventative Therapy With Coronary Computed Tomographic Angiography: Added Value Beyond Simple Risk Calculators?J Am Coll Cardiol. 2016 Oct 4;68(14):1603-4. doi: 10.1016/j.jacc.2016.06.065. J Am Coll Cardiol. 2016. PMID: 27687205 No abstract available.
-
Reply: Enhanced Preventative Therapy With Coronary Computed Tomographic Angiography: Added Value Beyond Simple Risk Calculators? AND Primum Non Nocere: Old Principle Revisited.J Am Coll Cardiol. 2016 Oct 4;68(14):1604-5. doi: 10.1016/j.jacc.2016.07.738. J Am Coll Cardiol. 2016. PMID: 27687206 No abstract available.
References
-
- Fihn S.D., Gardin J.M., Abrams J., et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2012;60:e44–e164. - PubMed
-
- Montalescot G., Sechtem U., Achenbach S., et al. 2013 ESC guidelines on the management of stable coronary artery disease: the Task Force on the Management of Stable Coronary Artery Disease of the European Society of Cardiology. Eur Heart J. 2013;34:2949–3003. - PubMed
-
- The SCOT-HEART Investigators CT coronary angiography in patients with suspected angina due to coronary heart disease (SCOT-HEART): an open-label, parallel-group, multicentre trial. Lancet. 2015;385:2383–2391. - PubMed
-
- Newby D.E., Williams M.C., Flapan A.D., et al. Role of multidetector computed tomography in the diagnosis and management of patients attending the rapid access chest pain clinic, The Scottish computed tomography of the heart (SCOT-HEART) trial: study protocol for randomized controlled trial. Trials. 2012;13:184. - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
