

CT and MR imaging of odontoid abnormalities: A pictorial review
- PMID: 27081234
- PMCID: PMC4813060
- DOI: 10.4103/0971-3026.178358
CT and MR imaging of odontoid abnormalities: A pictorial review
Abstract
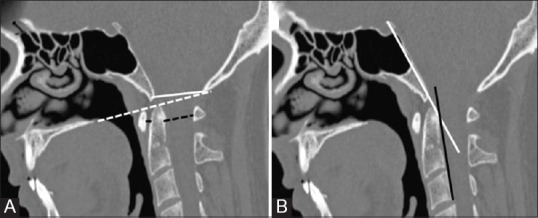
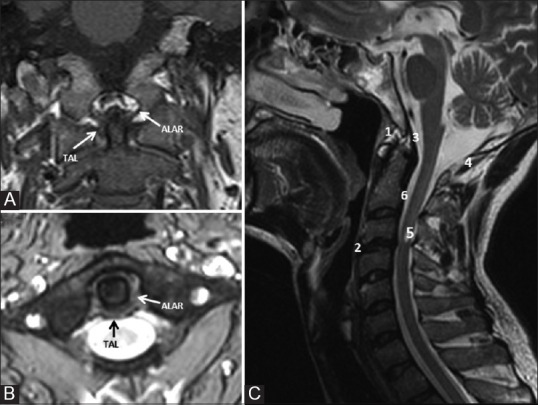
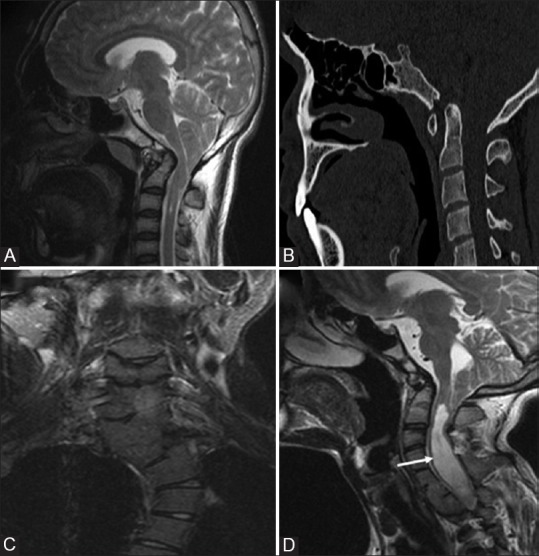
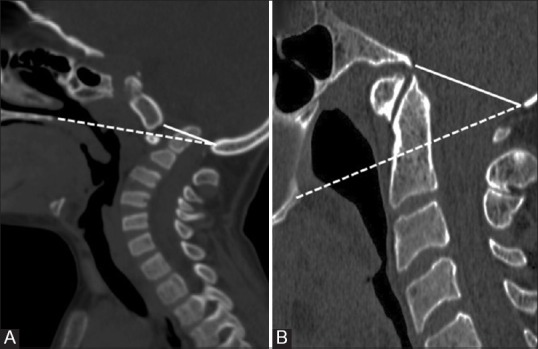
Odontoid process is the central pillar of the craniovertebral junction. Imaging of this small structure continues to be a challenge for the radiologists due to complex bony and ligamentous anatomy. A wide range of developmental and acquired abnormalities of odontoid have been identified. Their accurate radiologic evaluation is important as different lesions have markedly different clinical course, patient management, and prognosis. This article seeks to provide knowledge for interpreting appearances of odontoid on computed tomography (CT) and magnetic resonance imaging (MRI) with respect to various disease processes, along with providing a quick review of the embryology and relevant anatomy.
Keywords: Anterior longitudinal ligament; atlanto-axial dislocation; atlanto-dental interval; basilar invagination; computed tomography; cranio-vertebral junction; fracture; magnetic resonance imaging; odontoid; posterior longitudinal ligament; transverse atlantal ligament.
Figures

References
-
- Hensinger RN, Fielding JW, Hawkins RJ. Congenital anomalies of the odontoid process. Orthop Clin North Am. 1978;9:901–12. - PubMed
-
- Erbengi A, Oge HK. Congenital malformations of the craniovertebral junction: Classification and surgical treatment. Acta Neurochir (Wien) 1994;127:180–5. - PubMed
-
- Redlund-Johnell I, Pettersson H. Radiographic measurements of thecranio-vertebral region. Designed for evaluation of abnormalities in rheumatoidarthritis. Acta Radiol Diagn (Stockh) 1984;25:23–8. - PubMed
-
- McRae DL. Bony abnormalities in the region of the foramen magnum: Correlation of the anatomic and neurologic findings. Acta Radiol. 1953;40:335–54. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources