

A case report on paraneoplastic encephalitis associated with astrocytoma - An unknown entity
- PMID: 27081239
- PMCID: PMC4813065
- DOI: 10.4103/0971-3026.178365
A case report on paraneoplastic encephalitis associated with astrocytoma - An unknown entity
Abstract
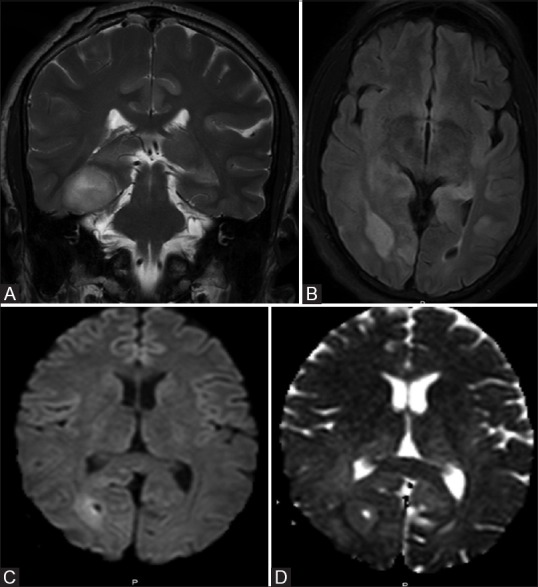
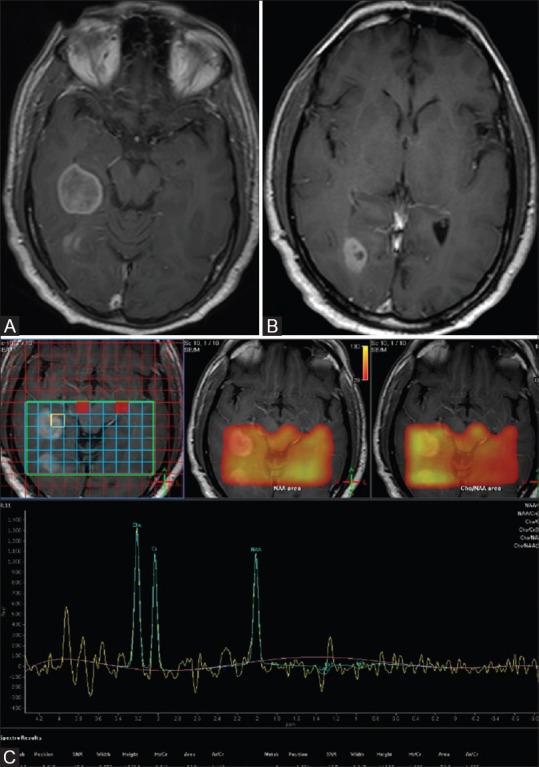
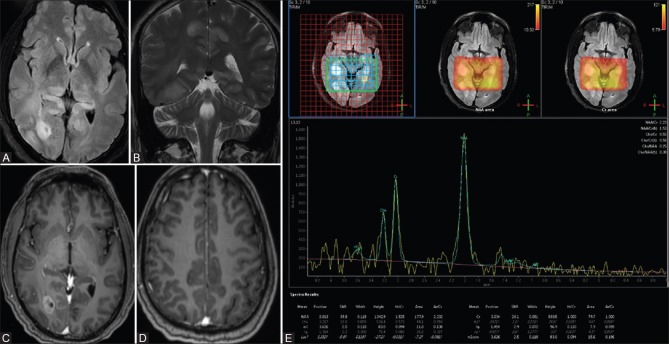
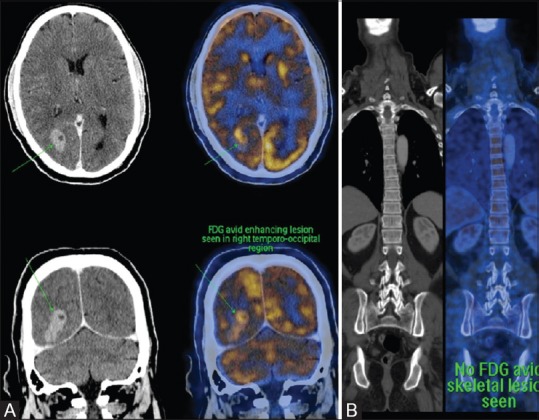
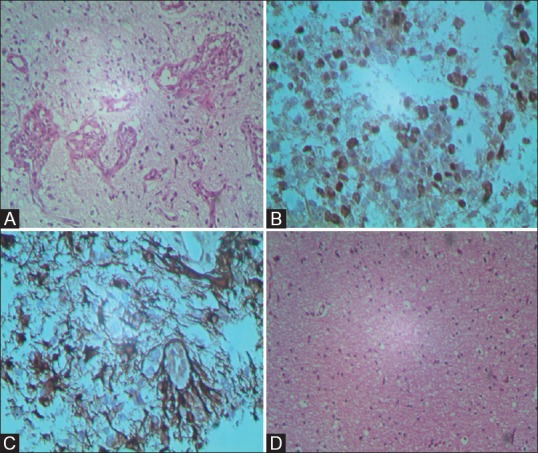
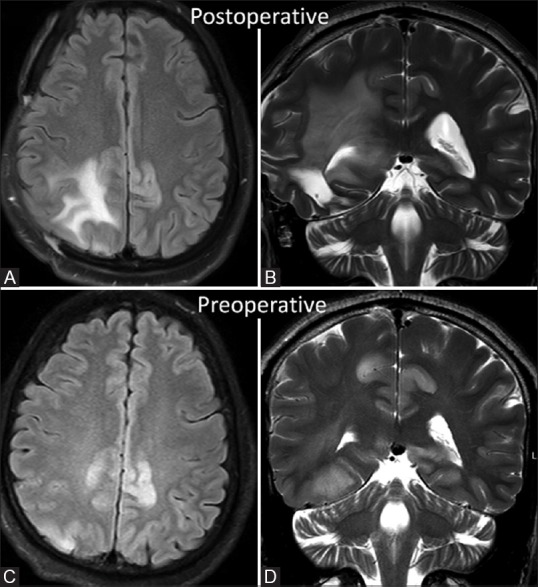
Paraneoplastic encephalitis is a multifocal inflammatory disorder of the central nervous system (CNS) that is associated with remote neoplasias. The most common malignancy associated with it is bronchial carcinoma, typically small cell carcinoma of lung. It has never been described in association with intracranial neoplasm. We present and discuss the clinical, radiological, and histopathological findings of paraneoplastic encephalitis with intracranial space-occupying lesions (SOLs) in a 55-year-old man. He was thoroughly investigated and biopsy revealed presence of astrocytoma with changes of paraneoplastic encephalitis.
Keywords: Astrocytoma; limbic encephalitis; paraneoplastic encephalitis.
Figures
References
-
- Seki M, Suzuki S, Ishii K, Izawa Y, Takahashi S, Toyama Y, et al. Differential diagnosis between intracranial dissemination of spinal cord astrocytoma and paraneoplastic limbic encephalitis. Intern Med. 2012;51:321–4. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources