

A tunable delivery platform to provide local chemotherapy for pancreatic ductal adenocarcinoma
- PMID: 27082874
- PMCID: PMC4849535
- DOI: 10.1016/j.biomaterials.2016.03.044
A tunable delivery platform to provide local chemotherapy for pancreatic ductal adenocarcinoma
Abstract
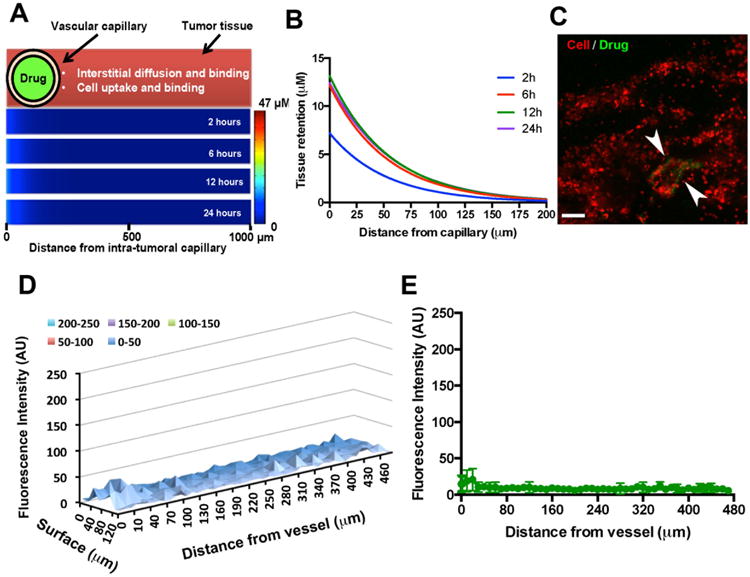
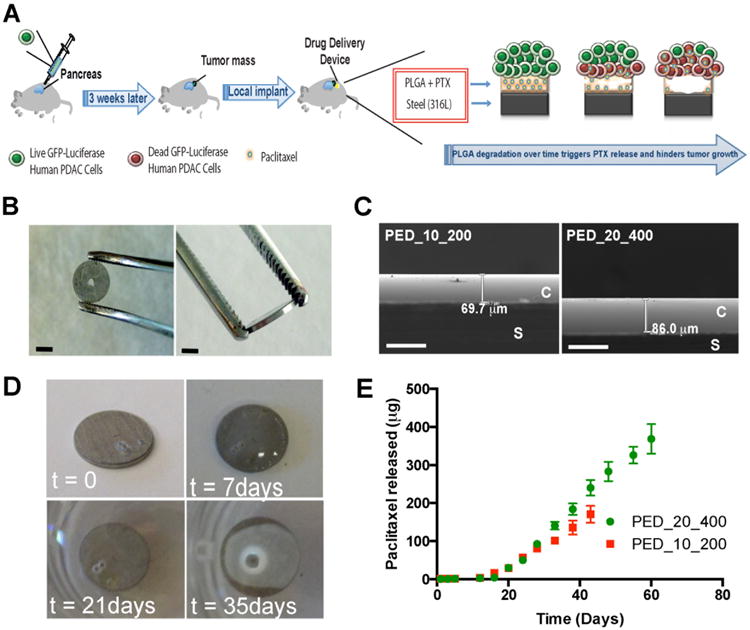
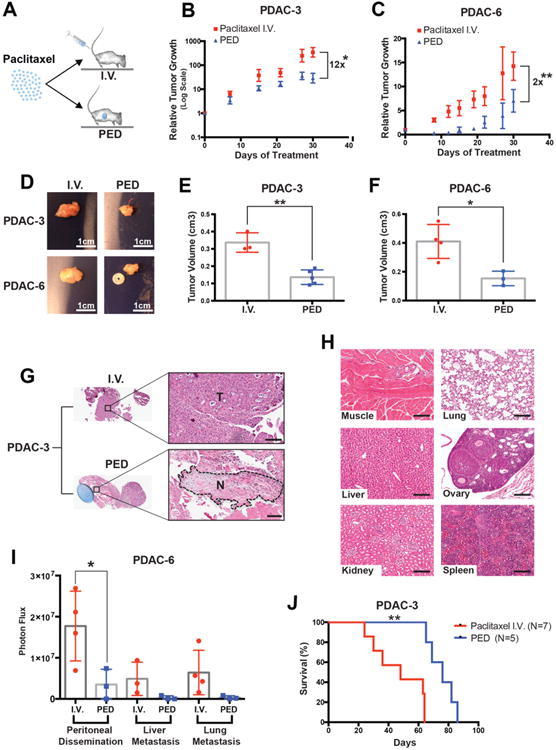
Pancreatic ductal adenocarcinoma (PDAC) is one of the most devastating and painful cancers. It is often highly resistant to therapy owing to inherent chemoresistance and the desmoplastic response that creates a barrier of fibrous tissue preventing transport of chemotherapeutics into the tumor. The growth of the tumor in pancreatic cancer often leads to invasion of other organs and partial or complete biliary obstruction, inducing intense pain for patients and necessitating tumor resection or repeated stenting. Here, we have developed a delivery device to provide enhanced palliative therapy for pancreatic cancer patients by providing high concentrations of chemotherapeutic compounds locally at the tumor site. This treatment could reduce the need for repeated procedures in advanced PDAC patients to debulk the tumor mass or stent the obstructed bile duct. To facilitate clinical translation, we created the device out of currently approved materials and drugs. We engineered an implantable poly(lactic-co-glycolic)-based biodegradable device that is able to linearly release high doses of chemotherapeutic drugs for up to 60 days. We created five patient-derived PDAC cell lines and tested their sensitivity to approved chemotherapeutic compounds. These in vitro experiments showed that paclitaxel was the most effective single agent across all cell lines. We compared the efficacy of systemic and local paclitaxel therapy on the patient-derived cell lines in an orthotopic xenograft model in mice (PDX). In this model, we found up to a 12-fold increase in suppression of tumor growth by local therapy in comparison to systemic administration and reduce retention into off-target organs. Herein, we highlight the efficacy of a local therapeutic approach to overcome PDAC chemoresistance and reduce the need for repeated interventions and biliary obstruction by preventing local tumor growth. Our results underscore the urgent need for an implantable drug-eluting platform to deliver cytotoxic agents directly within the tumor mass as a novel therapeutic strategy for patients with pancreatic cancer.
Keywords: Chemoresistance; Local delivery; Paclitaxel; Pancreatic cancer; Patient-derived xenograft; Poly(lactic-co-glycolic acid).
Copyright © 2016 Elsevier Ltd. All rights reserved.
Figures



References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
