

Impact of Nurse-Led, Multidisciplinary Home-Based Intervention on Event-Free Survival Across the Spectrum of Chronic Heart Disease: Composite Analysis of Health Outcomes in 1226 Patients From 3 Randomized Trials
- PMID: 27083509
- PMCID: PMC4857795
- DOI: 10.1161/CIRCULATIONAHA.116.020730
Impact of Nurse-Led, Multidisciplinary Home-Based Intervention on Event-Free Survival Across the Spectrum of Chronic Heart Disease: Composite Analysis of Health Outcomes in 1226 Patients From 3 Randomized Trials
Abstract
Background: We sought to determine the overall impact of a nurse-led, multidisciplinary home-based intervention (HBI) adapted to hospitalized patients with chronic forms of heart disease of varying types.
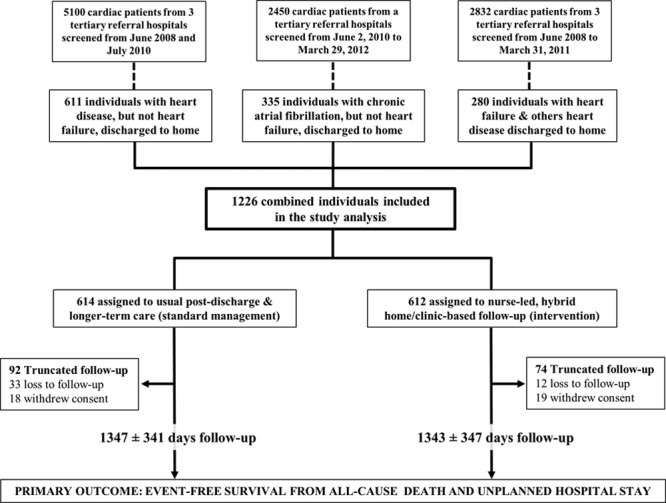
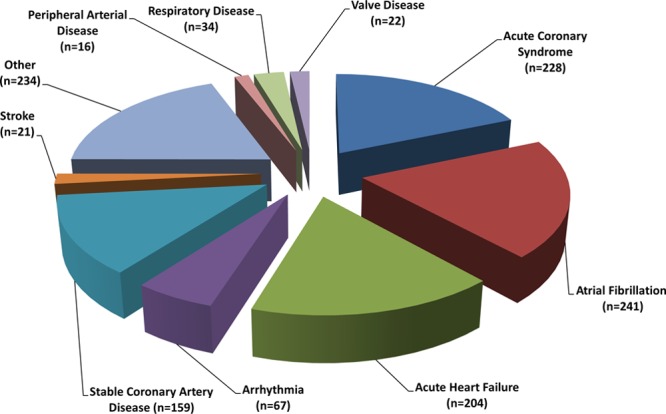
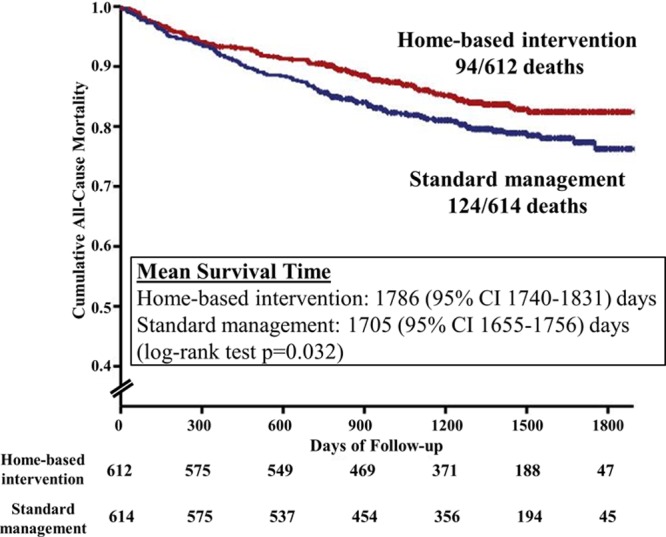
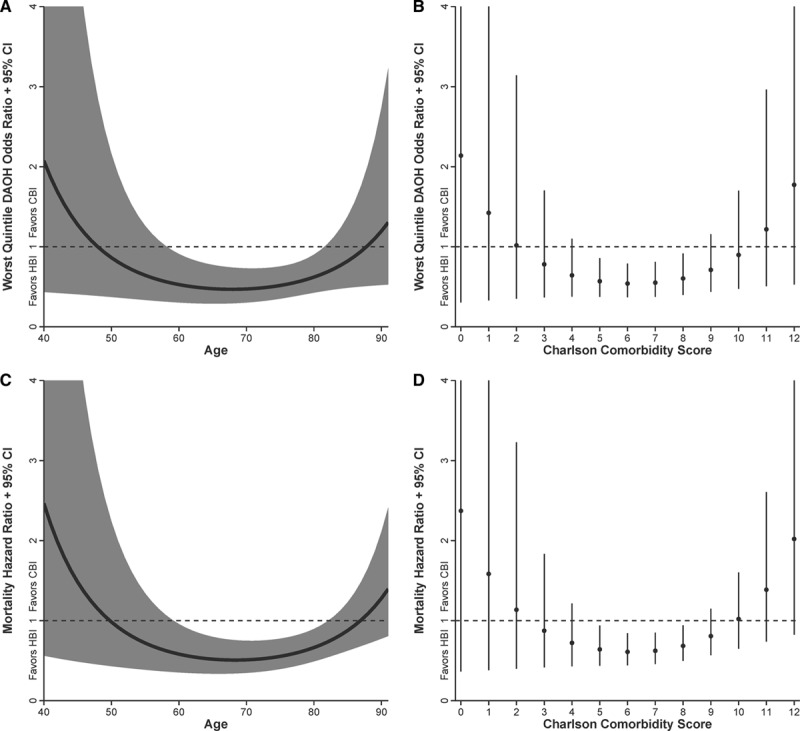
Methods and results: Prospectively planned, combined, secondary analysis of 3 randomized trials (1226 patients) of HBI were compared with standard management. Hospitalized patients presenting with heart disease but not heart failure, atrial fibrillation but not heart failure, and heart failure, as well, were recruited. Overall, 612 and 614 patients, respectively, were allocated to a home visit 7 to 14 days postdischarge by a cardiac nurse with follow-up and multidisciplinary support according to clinical need or standard management. The primary outcome of days-alive and out-of-hospital was examined on an intention-to-treat basis. During 1371 days (interquartile range, 1112-1605) of follow-up, 218 patients died and 17 917 days of hospital stay were recorded. In comparison with standard management, HBI patients achieved significantly prolonged event-free survival (90.1% [95% confidence interval, 88.2-92.0] versus 87.2% [95% confidence interval, 85.1-89.3] days-alive and out-of-hospital; P=0.020). This reflected less all-cause mortality (adjusted hazard ratio, 0.67; 95% confidence interval, 0.50-0.88; P=0.005) and unplanned hospital stay (median, 0.22 [interquartile range, 0-1.3] versus 0.36 [0-2.1] days/100 days follow-up; P=0.011). Analyses of the differential impact of HBI on all-cause mortality showed significant interactions (characterized by U-shaped relationships) with age (P=0.005) and comorbidity (P=0.041); HBI was most effective for those aged 60 to 82 years (59%-65% of individual trial cohorts) and with a Charlson Comorbidity Index Score of 5 to 8 (36%-61%).
Conclusions: These data provide further support for the application of postdischarge HBI across the full spectrum of patients being hospitalized for chronic forms of heart disease.
Clinical trial registration: URL: http://www.anzctr.org.au. Unique identifiers: 12610000221055, 12608000022369, 12607000069459.
Keywords: case management; heart diseases; mortality; outcome assessment (health care); patient readmission; secondary prevention.
© 2016 The Authors.
Figures
Comment in
-
Disease Management Programs in Cardiology: Extending the Success in Failure.Circulation. 2016 May 10;133(19):1836-7. doi: 10.1161/CIRCULATIONAHA.116.022480. Epub 2016 Apr 15. Circulation. 2016. PMID: 27083508 No abstract available.
References
-
- Sochalski J, Jaarsma T, Krumholz HM, Laramee A, McMurray JJ, Naylor MD, Rich MW, Riegel B, Stewart S. What works in chronic care management: the case of heart failure. Health Aff (Millwood) 2009;28:179–189. doi: 10.1377/hlthaff.28.1.179. - PubMed
-
- Anderson L, Oldridge N, Thompson DR, Zwisler AD, Rees K, Martin N, Taylor RS. Exercise-based cardiac rehabilitation for coronary heart disease: Cochrane systematic review and meta-analysis. J Am Coll Cardiol. 2016;67:1–12. doi: 10.1016/j.jacc.2015.10.044. - PubMed
-
- McAlister FA, Stewart S, Ferrua S, McMurray JJ. Multidisciplinary strategies for the management of heart failure patients at high risk for admission: a systematic review of randomized trials. J Am Coll Cardiol. 2004;44:810–819. doi: 10.1016/j.jacc.2004.05.055. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
