

EuroQol Protocols for Time Trade-Off Valuation of Health Outcomes
- PMID: 27084198
- PMCID: PMC5023738
- DOI: 10.1007/s40273-016-0404-1
EuroQol Protocols for Time Trade-Off Valuation of Health Outcomes
Abstract
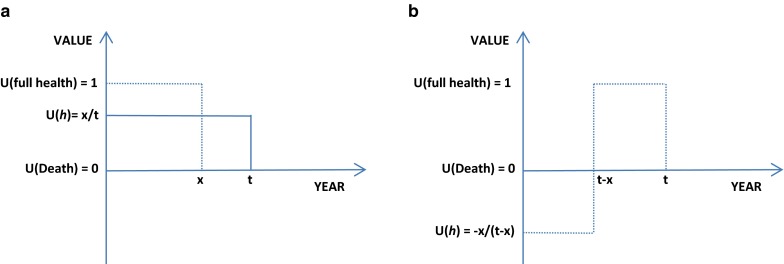
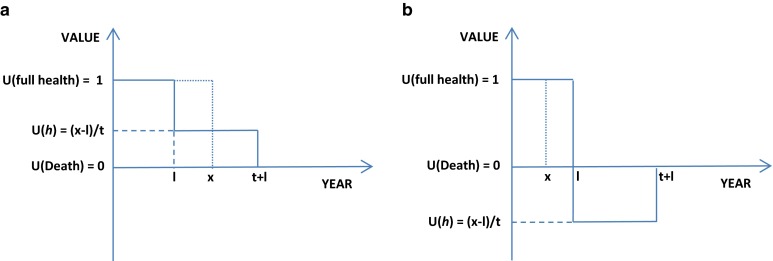
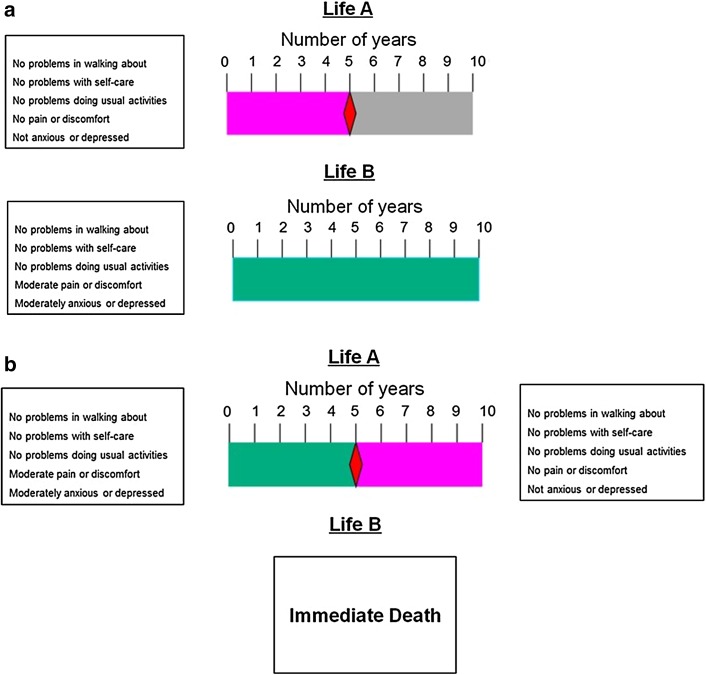
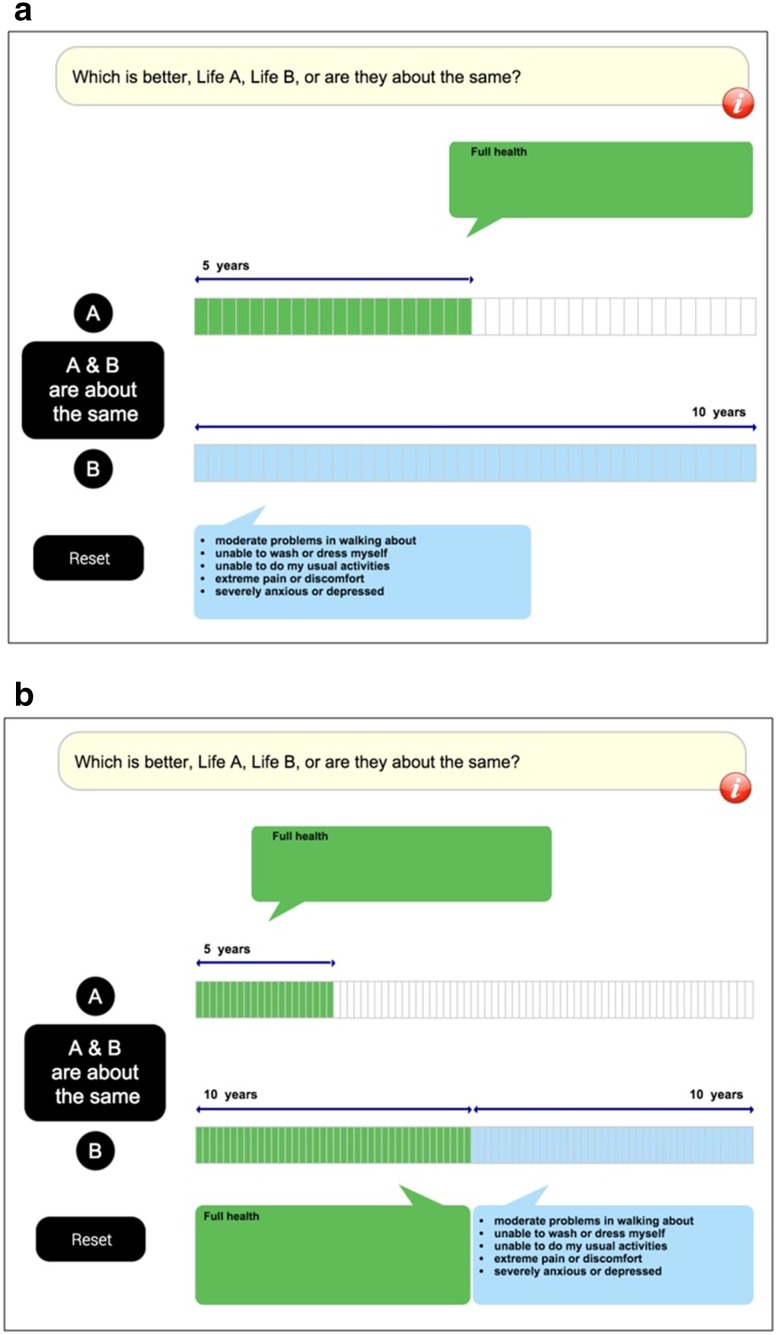
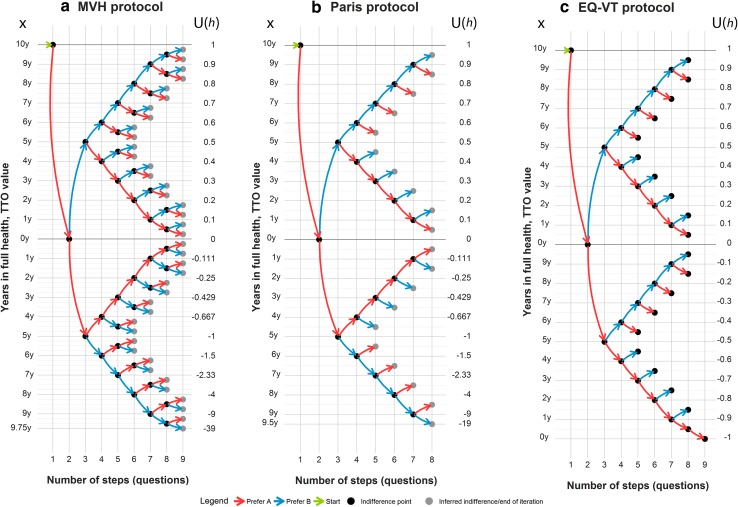
The time trade-off (TTO) valuation technique is widely used to determine utility values of health outcomes to inform quality-adjusted life-year (QALY) calculations for use in economic evaluation. Protocols for implementing TTO vary in aspects such as the trade-off framework, iteration procedure and its administration model and method, training of respondents and interviewers, and quality control of data collection. The most widely studied and utilized TTO valuation protocols are the Measurement and Valuation of Health (MVH) protocol, the Paris protocol and the EuroQol Valuation Technology (EQ-VT) protocol, all developed by members of the EuroQol Group. The MVH protocol and its successor, the Paris protocol, were developed for valuation of EQ-5D-3L health states. Both protocols were designed for a trained interviewer to elicit preferences from a respondent using the conventional TTO framework with a fixed time horizon of 10 years and an iteration procedure combining bisection and titration. Developed for valuation of EQ-5D-5L health states, the EQ-VT protocol adopted a composite TTO framework and made use of computer technology to facilitate data collection. Training and monitoring of interviewers and respondents is a pivotal component of the EQ-VT protocol. Research is underway aiming to further improve the EuroQol protocols, which form an important basis for the current practice of health technology assessment in many countries.
Conflict of interest statement
Compliance with Ethical Standards Funding This work is partially supported by the EuroQol Research Foundation. Conflict of interest All authors are members of the EuroQol Group. Disclaimer The views of the authors expressed in the paper do not necessarily reflect the views of the EuroQol Group. Part of the content of this paper was presented in a workshop at the 2014 International Society for Pharmacoeconomics and Outcomes Research (ISPOR) Asia–Pacific Congress in Beijing, China.
Figures
References
-
- Brazier J, Ratcliffe J, Salomon JA, Tsuchiya A. Measuring and valuing health benefits for economic evaluation. Oxford: Oxford University Press; 2007.
-
- Pliskin JS, Shepard DS, Weinstein MC. Utility functions for life years and health status. Oper Res. 1980;28:206–224.
-
- Ryan M, Scott DA, Reeves C, Bate A, van Teijlingen ER, Russell EM, Napper M, Robb CM. Eliciting public preferences for healthcare: a systematic review of techniques. Health Technol Assess. 2001;5(5):1–186. - PubMed
-
- Bleichrodt H, Johannesson M. Standard gamble, time trade-off and rating scale: experimental results on the ranking properties of QALYs. J Health Econ. 1997;16(2):155–175. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
