

Pharmaceutical treatments to prevent recurrence of endometriosis following surgery: a model-based economic evaluation
- PMID: 27084280
- PMCID: PMC4838778
- DOI: 10.1136/bmjopen-2015-010580
Pharmaceutical treatments to prevent recurrence of endometriosis following surgery: a model-based economic evaluation
Abstract
Objective: Conduct an economic evaluation based on best currently available evidence comparing alternative treatments levonorgestrel-releasing intrauterine system, depot-medroxyprogesterone acetate, combined oral contraceptive pill (COCP) and 'no treatment' to prevent recurrence of endometriosis after conservative surgery in primary care, and to inform the design of a planned trial-based economic evaluation.
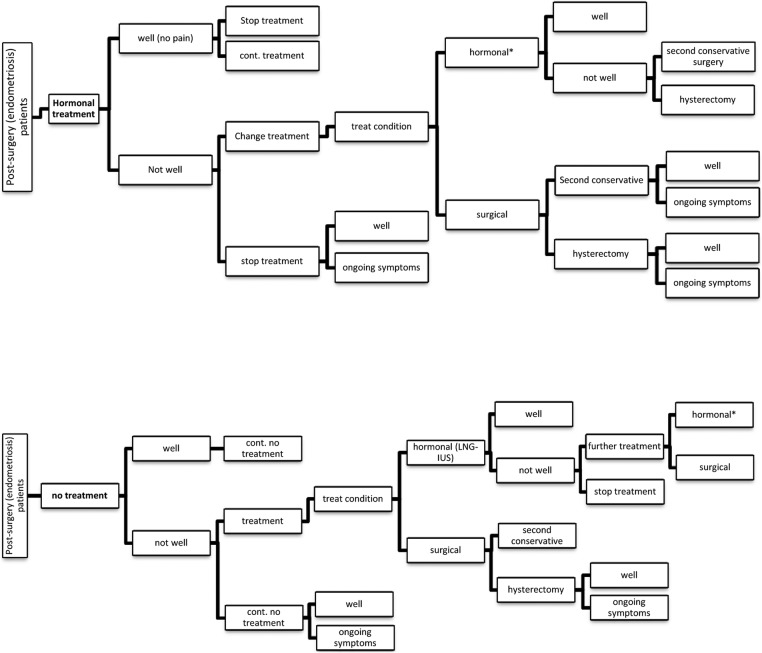
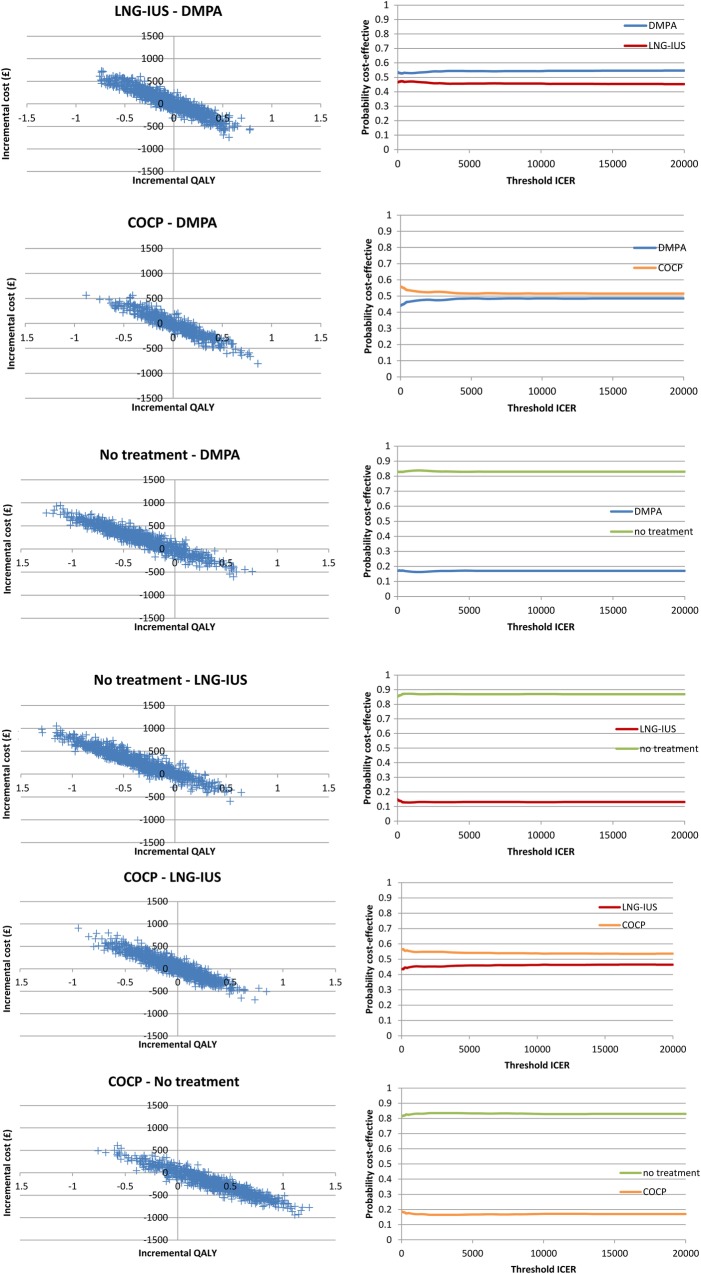
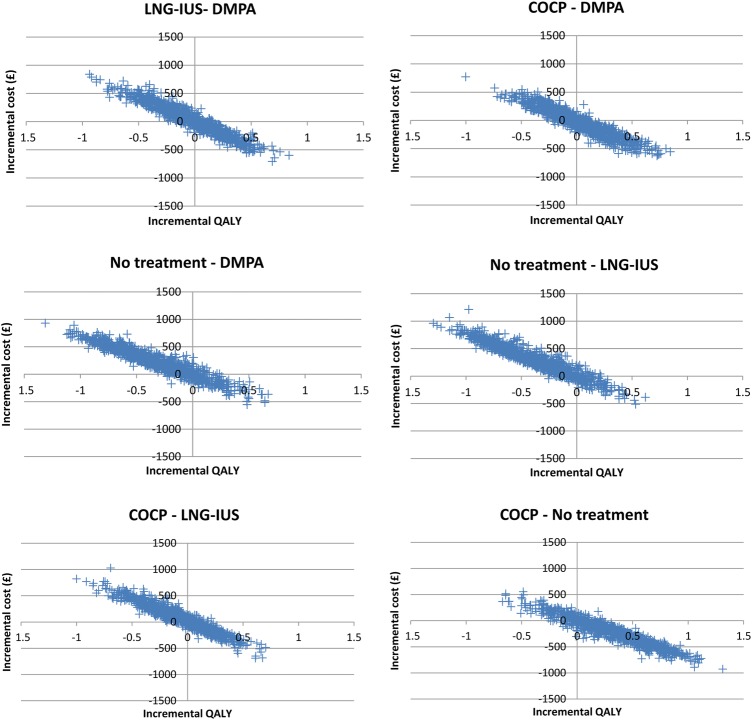
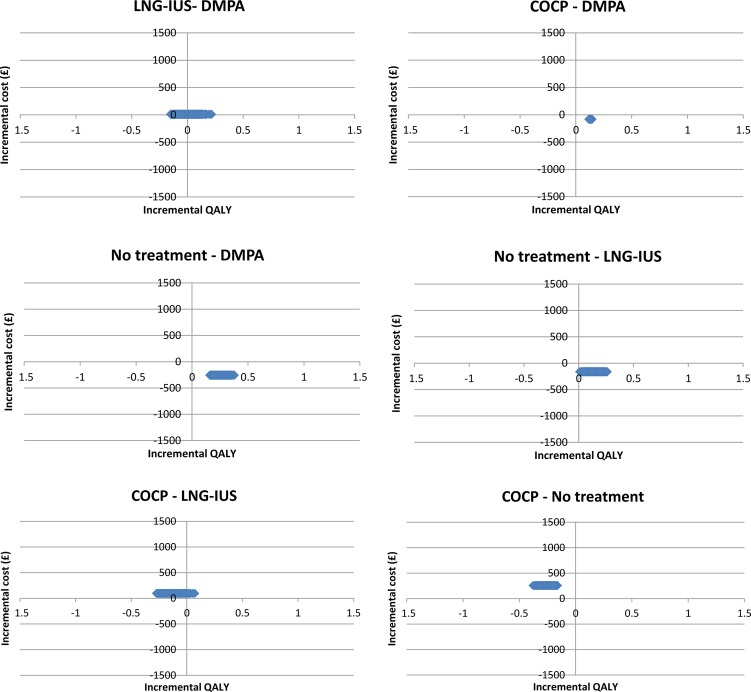
Methods: We developed a state transition (Markov) model with a 36-month follow-up. The model structure was informed by a pragmatic review and clinical experts. The economic evaluation adopted a UK National Health Service perspective and was based on an outcome of incremental cost per quality-adjusted life year (QALY). As available data were limited, intentionally wide distributions were assigned around model inputs, and the average costs and outcome of the probabilistic sensitivity analyses were reported.
Results: On average, all strategies were more expensive and generated fewer QALYs compared to no treatment. However, uncertainty attributing to the transition probabilities affected the results. Inputs relating to effectiveness, changes in treatment and the time at which the change is made were the main causes of uncertainty, illustrating areas where robust and specific data collection is required.
Conclusions: There is currently no evidence to support any treatment being recommended to prevent the recurrence of endometriosis following conservative surgery. The study highlights the importance of developing decision models at the outset of a trial to identify data requirements to conduct a robust post-trial analysis.
Keywords: OBSTETRICS.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures
References
-
- ESHRE—European Society of Human Reproduction and Embryology. Management of women with endometriosis. ESHRE Guideline development group 2013. http://www.eshre.eu/~/media/Files/ESHRE%20guideline%20on%20endometriosis...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical