

A Global Risk Score (GRS) to Simultaneously Predict Early and Late Tumor Recurrence Risk after Resection of Hepatocellular Carcinoma
- PMID: 27084430
- PMCID: PMC4833966
- DOI: 10.1016/j.tranon.2016.02.003
A Global Risk Score (GRS) to Simultaneously Predict Early and Late Tumor Recurrence Risk after Resection of Hepatocellular Carcinoma
Abstract
Objectives: Recurrence of hepatocellular carcinoma can arise from the primary tumor ("early recurrence") or de novo from tumor formation in a cirrhotic environment ("late recurrence"). We aimed to develop one simple gene expression score applicable in both the tumor and the surrounding liver that can predict the recurrence risk.
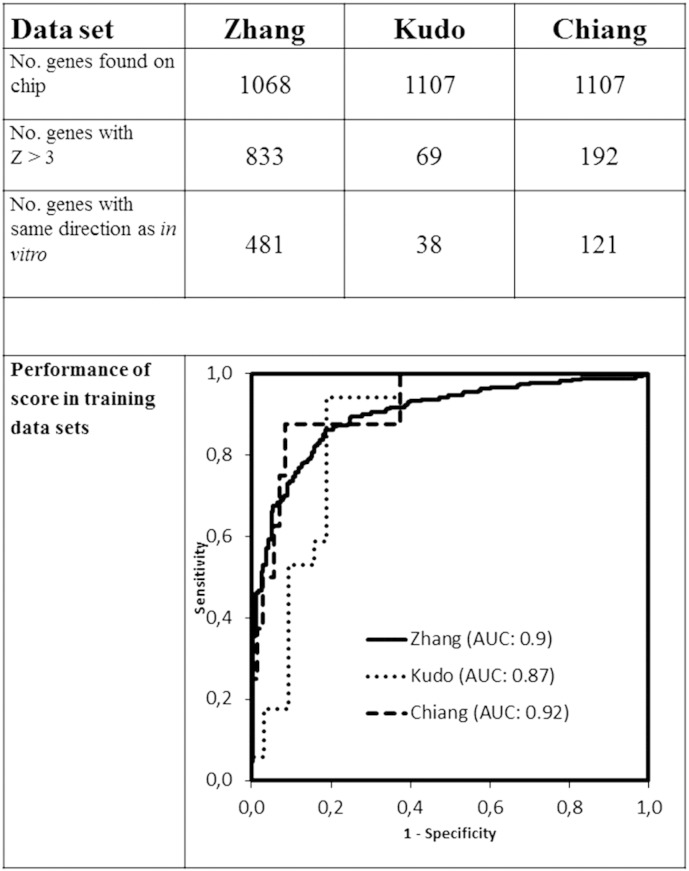
Methods: We determined differentially expressed genes in a cell model of cancer aggressiveness. These genes were first validated in three large published data sets of hepatocellular carcinoma from which we developed a seven-gene risk score.
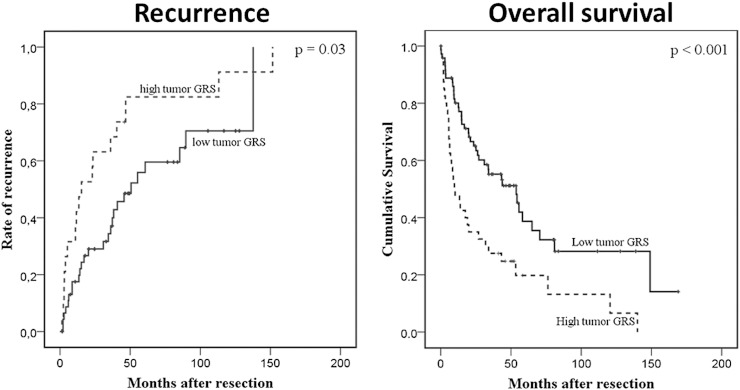
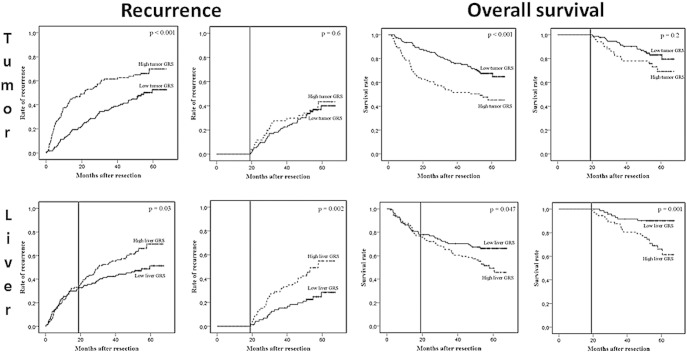
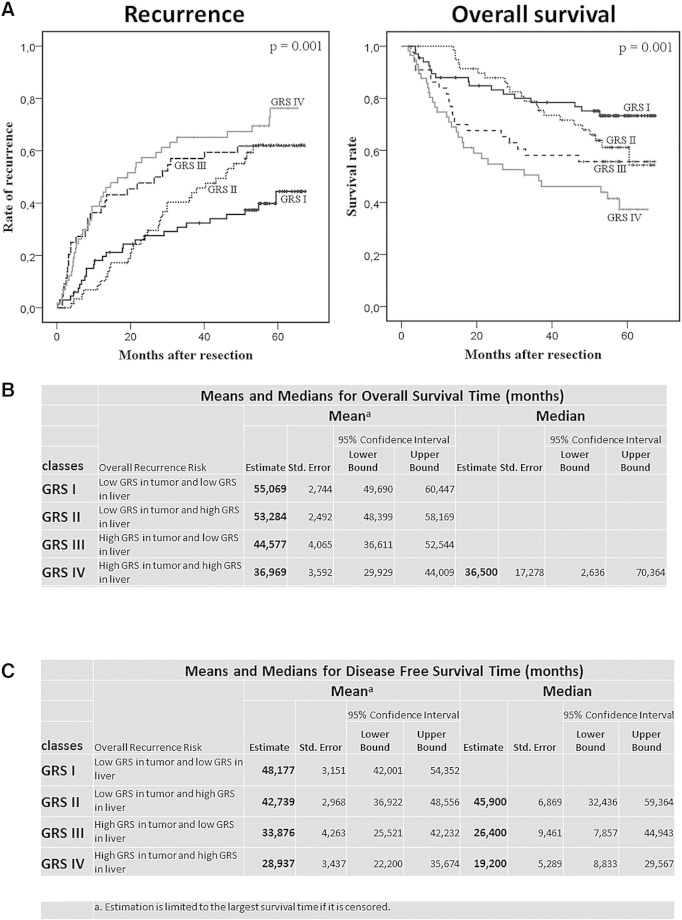
Results: The gene score was applied on two independent large patient cohorts. In the first cohort, with only tumor data available, it could predict the recurrence risk at 3 years after resection (68 ± 10% vs 35 ± 7%, P = .03). In the second cohort, when applied on the tumor, this gene score predicted early recurrence (62 ± 5% vs 37 ± 4%, P < .001), and when applied on the surrounding liver tissue, the same genes also correlated with late recurrence. Four patient classes with each different time patterns and rates of recurrence could be identified based on combining tumor and liver scores. In a multivariate Cox regression analysis, our gene score remained significantly associated with recurrence, independent from other important cofactors such as disease stage (P = .007).
Conclusions: We developed a Global Risk Score that is able to simultaneously predict the risk of early recurrence when applied on the tumor itself, as well as the risk of late recurrence when applied on the surrounding liver tissue.
Copyright © 2015. Published by Elsevier Inc.
Figures
References
-
- Poon RT, Fan ST, Ng IO, Wong J. Different risk factors and prognosis for early and late intrahepatic recurrence after resection of hepatocellular carcinoma. Cancer. 2000;89:500–507. - PubMed
-
- Llovet JM, Di Bisceglie AM, Bruix J, Kramer BS, Lencioni R, Zhu AX, Sherman M, Schwartz M, Lotze M, Talwalkar J, Gores GJ, Panel of Experts in HCC-Design Clinical Trials Design and endpoints of clinical trials in hepatocellular carcinoma. J Natl Cancer Inst. 2008;100(10):698–711. [ http://jnci.oxfordjournals.org/content/100/10/698.long] - PubMed
-
- Verslype C, Van Cutsem E, Dicato M, Arber N, Berlin JD, Cunningham D, De Gramont A, Diaz-Rubio E, Ducreux M, Gruenberger T. The management of hepatocellular carcinoma. Current expert opinion and recommendations derived from the 10th World Congress on Gastrointestinal Cancer, Barcelona, 2008. Ann Oncol. 2009;20(Suppl 7):vii1–vii6. [ http://annonc.oxfordjournals.org/content/20/suppl_7/vii1.long] - PubMed
-
- Roayaie S, Jibara G, Tabrizian P, Park JW, Yang J, Yan L, Schwartz M, Han G, Izzo F, Chen M. The role of hepatic resection in the treatment of hepatocellular cancer. Hepatology. 2015;62(2):440–451. [ http://onlinelibrary.wiley.com/doi/10.1002/hep.27745/full] - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
