

Membranous Nephropathy: A Journey From Bench to Bedside
- PMID: 27085376
- PMCID: PMC4921260
- DOI: 10.1053/j.ajkd.2016.01.030
Membranous Nephropathy: A Journey From Bench to Bedside
Abstract
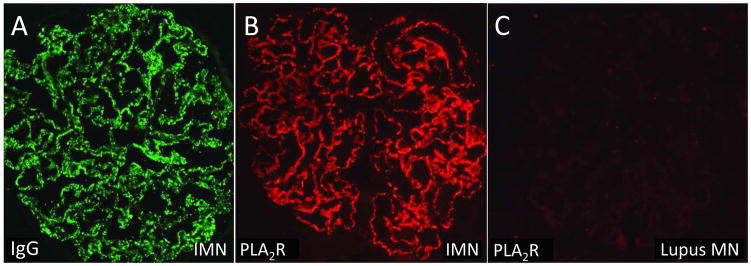
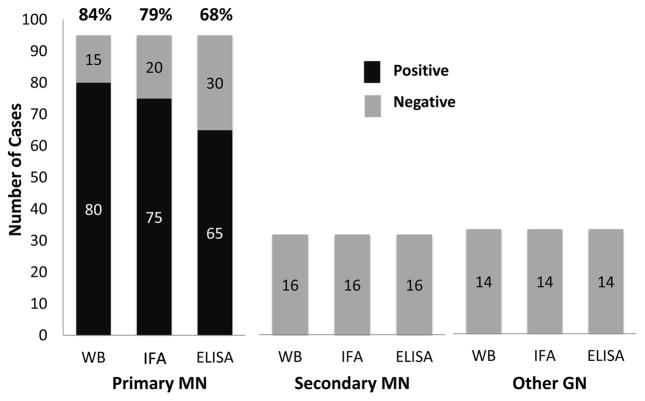
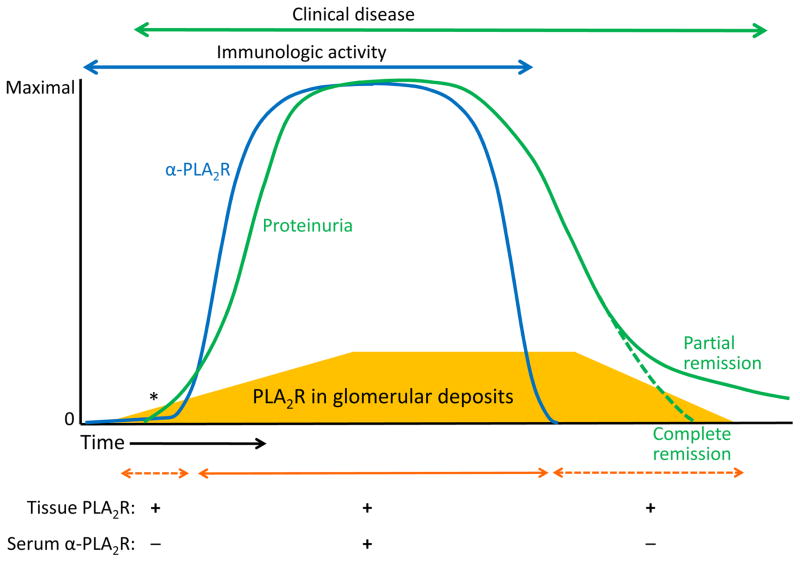
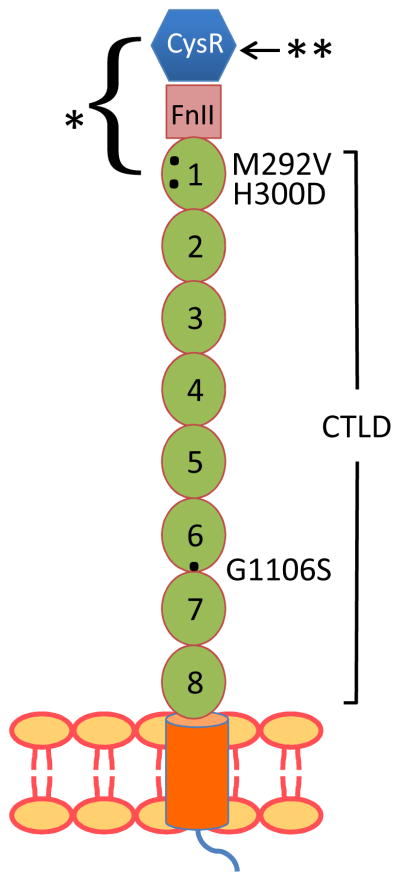
Lessons from an animal model that faithfully resembles human membranous nephropathy (MN) have informed our understanding of the pathogenesis of this organ-specific autoimmune disease and common cause of nephrotic syndrome. After it was established that the subepithelial immune deposits that characterize experimental MN form in situ when circulating antibodies bind to an intrinsic podocyte antigen, it was merely a matter of time before the human antigen was identified. The M-type phospholipase A2 receptor 1 (PLA2R) represents the major target antigen in primary MN, and thrombospondin type 1 domain-containing 7A (THSD7A) was more recently identified as a minor antigen. Serologic tests for anti-PLA2R and kidney biopsy specimen staining for PLA2R show >90% specificity and 70% to 80% sensitivity for the diagnosis of primary MN in most populations. The assays distinguish most cases of primary MN from MN associated with other systemic diseases, and sequential anti-PLA2R titers are useful to monitor treatment response. A positive pretransplantation test result for anti-PLA2R is also helpful for predicting the risk for posttransplantation recurrence. Identification of target epitopes within PLA2R and the genetic association of primary MN with class II major histocompatibility and PLA2R1 variants are 2 additional examples of our evolving understanding of this disease.
Keywords: M-type phospholipase A(2) receptor 1 (PLA(2)R); Membranous nephropathy (MN); PLA2R1; class II major histocompatibility; epitope; genetic polymorphisms; nephrotic syndrome; organ-specific autoimmunity; post-transplant recurrent disease; thrombospondin type 1 domain-containing 7A (THSD7A).
Copyright © 2016 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Van Damme BJ, Fleuren GJ, Bakker WW, Vernier RL, Hoedemaeker PJ. Experimental glomerulonephritis in the rat induced by antibodies directed against tubular antigens. V. Fixed glomerular antigens in the pathogenesis of heterologous immune complex glomerulonephritis. Lab Invest. 1978;38(4):502–510. - PubMed
-
- Couser WG, Salant DJ. In situ immune complex formation and glomerular injury. Kidney Int. 1980;17(1):1–13. - PubMed
-
- Makker SP, Singh AK. Characterization of the antigen (gp600) of Heymann nephritis. Lab Invest. 1984;50(3):287–293. - PubMed
-
- Raychowdhury R, Nile JL, McCluskey RT, Smith JA. Autoimmune target in Heymann nephritis is a glycoprotein with homology to the LDL receptor. Science. 1989;244(4909):1163–1165. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
