

Improving the CAC Score by Addition of Regional Measures of Calcium Distribution: Multi-Ethnic Study of Atherosclerosis
- PMID: 27085449
- PMCID: PMC5055410
- DOI: 10.1016/j.jcmg.2016.03.001
Improving the CAC Score by Addition of Regional Measures of Calcium Distribution: Multi-Ethnic Study of Atherosclerosis
Abstract
Objectives: The aim of this study was to investigate whether inclusion of simple measures of calcified plaque distribution might improve the ability of the traditional Agatston coronary artery calcium (CAC) score to predict cardiovascular events.
Background: Agatston CAC scoring does not include information on the location and distributional pattern of detectable calcified plaque.
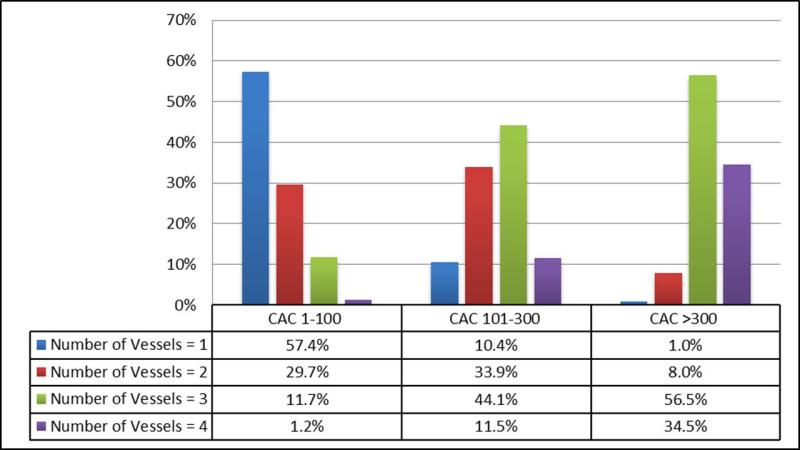
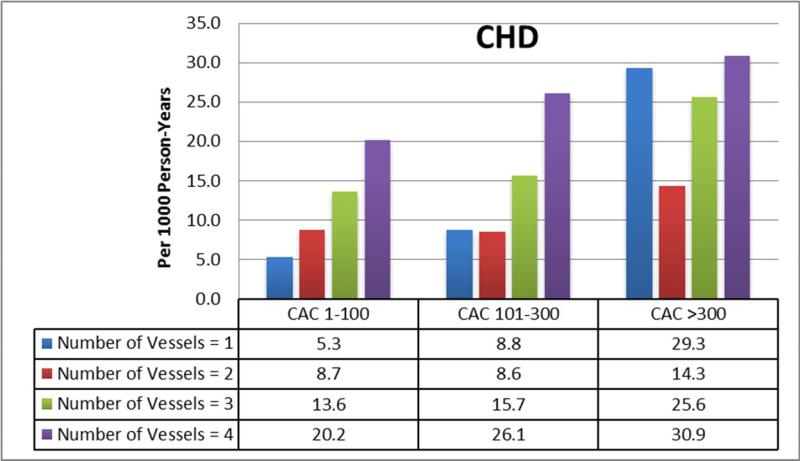
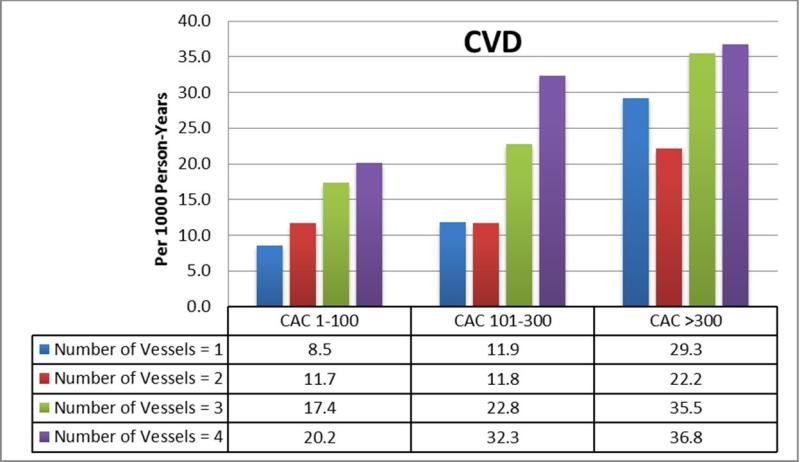
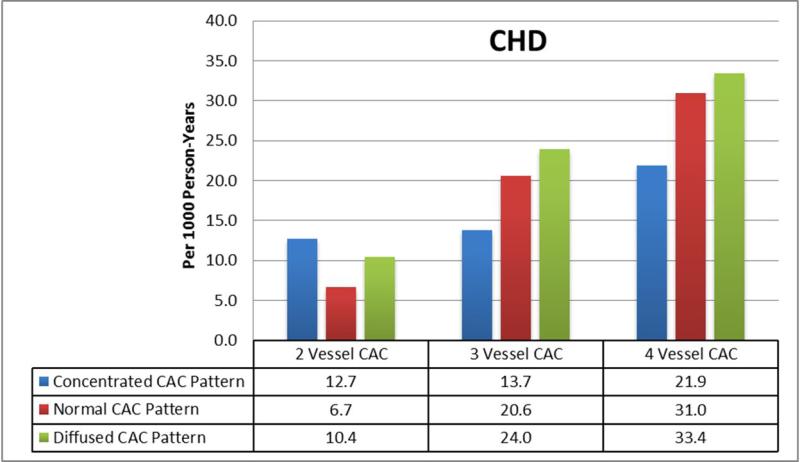
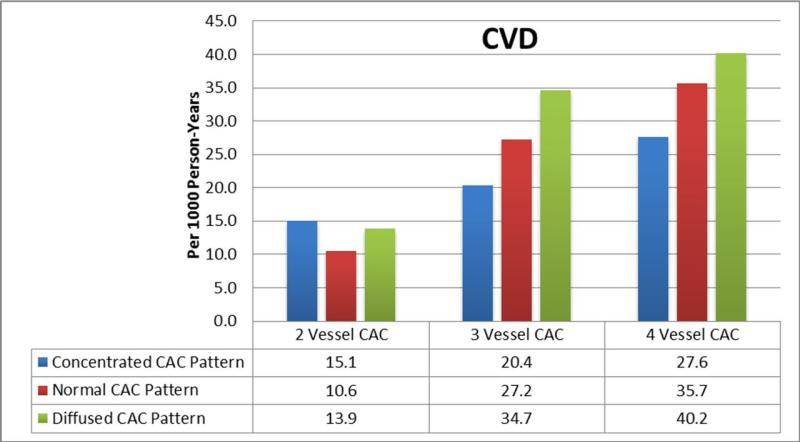
Methods: We studied 3,262 (50%) individuals with baseline CAC >0 from MESA (Multi-Ethnic Study of Atherosclerosis). Multivessel CAC was defined by the number of coronary vessels with CAC (scored 1 to 4, including the left main). The "diffusivity index" was calculated as: 1 - (CAC in most affected vessel/total CAC), and was used to group participants into concentrated and diffuse CAC patterns. Multivariable Cox proportional hazards regression, area under the curve, and net reclassification improvement analyses were performed for both coronary heart disease (CHD) and cardiovascular disease (CVD) events to assess whether measures of regional CAC distribution add to the traditional Agatston CAC score.
Results: Mean age of the population was 66 ± 10 years, with 42% women. Median follow-up was 10.0 (9.5 to 10.7) years and there were 368 CHD and 493 CVD events during follow-up. Considerable heterogeneity existed between CAC score group and number of vessels with CAC (p < 0.01). Addition of number of vessels with CAC significantly improved capacity to predict CHD and CVD events in survival analysis (hazard ratio: 1.9 to 3.5 for 4-vessel vs. 1-vessel CAC), area under the curve analysis (C-statistic improvement of 0.01 to 0.033), and net reclassification improvement analysis (category-less net reclassification improvement 0.10 to 0.45). Although a diffuse CAC pattern was associated with worse outcomes in participants with ≥2 vessels with CAC (hazard ratio: 1.33 to 1.41; p < 0.05), adding this variable to the Agatston CAC score and number of vessels with CAC did not further improve global risk prediction.
Conclusions: The number of coronary arteries with calcified plaque, indicating increasingly "diffuse" multivessel subclinical atherosclerosis, adds significantly to the traditional Agatston CAC score for the prediction of CHD and CVD events.
Keywords: cardiac computed tomography; risk prediction; risk stratification.
Copyright © 2016 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Coronary Artery Calcium Scanning: The Agatston Score and Beyond.JACC Cardiovasc Imaging. 2016 Dec;9(12):1417-1419. doi: 10.1016/j.jcmg.2016.05.020. JACC Cardiovasc Imaging. 2016. PMID: 27931526 No abstract available.
References
-
- Nasir K, Clouse M. Role of nonenhanced multidetector CT coronary artery calcium testing in asymptomatic and symptomatic individuals. Radiology. 2012;264:637–49. - PubMed
-
- Rumberger JA, Simons DB, Fitzpatrick LA, Sheedy PF, Schwartz RS. Coronary artery calcium area by electron-beam computed tomography and coronary atherosclerotic plaque area. A histopathologic correlative study. Circulation. 1995;92:2157–62. - PubMed
-
- Sangiorgi G, Rumberger JA, Severson A, et al. Arterial calcification and not lumen stenosis is highly correlated with atherosclerotic plaque burden in humans: a histologic study of 723 coronary artery segments using nondecalcifying methodology. J Am Coll Cardiol. 1998;31:126–33. - PubMed
-
- Agatston AS, Janowitz WR, Hildner FJ, et al. Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol. Mar. 1990;15:827–32. - PubMed
-
- Callister TQ, Cooil B, Raya SP, Lippolis NJ, Russo DJ, Raggi P. Coronary artery disease: improved reproducibility of calcium scoring with an electron-beam CT volumetric method. Radiology. 1998;208:807–14. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01 HC095161/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- L30 HL110027/HL/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
