

Magnetic Resonance Imaging-Guided Transcatheter Cavopulmonary Shunt
- PMID: 27085581
- PMCID: PMC5227171
- DOI: 10.1016/j.jcin.2016.01.032
Magnetic Resonance Imaging-Guided Transcatheter Cavopulmonary Shunt
Abstract
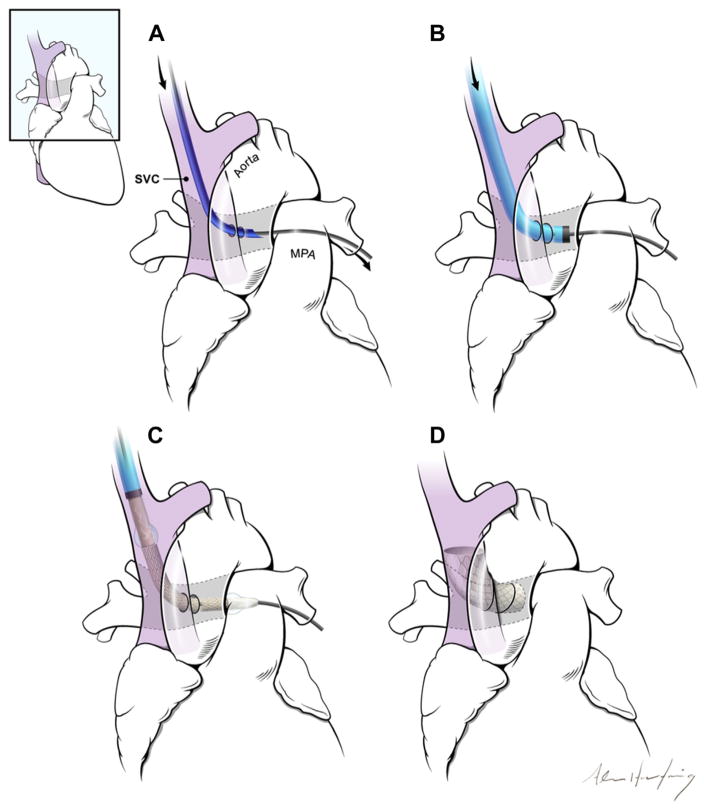
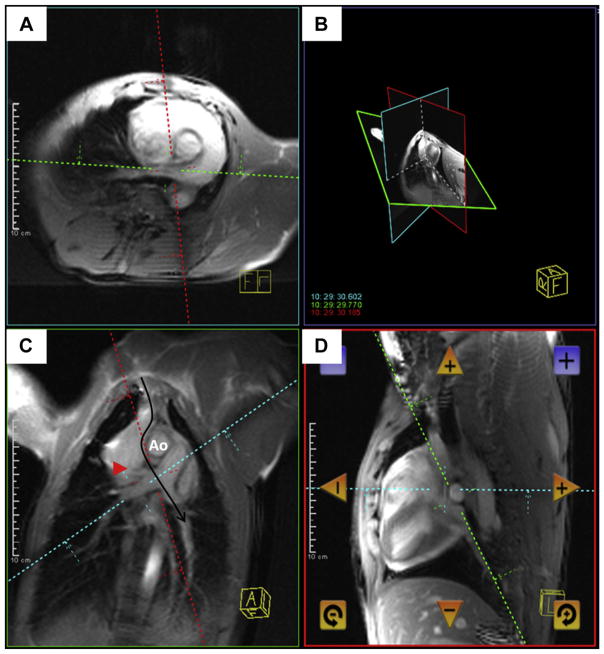
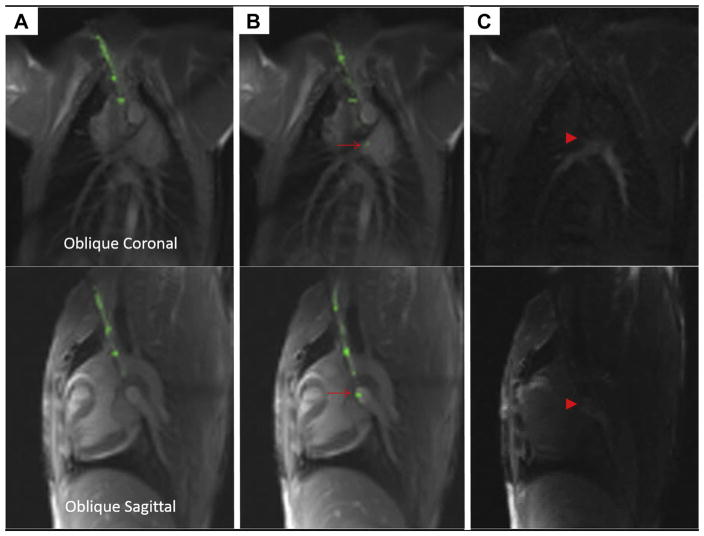
Objectives: The aim of this study was to test the hypothesis that real-time magnetic resonance imaging (MRI) would enable closed-chest percutaneous cavopulmonary anastomosis and shunt by facilitating needle guidance along a curvilinear trajectory, around critical structures, and between a superior vena cava "donor" vessel and a pulmonary artery "target."
Background: Children with single-ventricle physiology require multiple open heart operations for palliation, including sternotomies and cardiopulmonary bypass. The reduced morbidity of a catheter-based approach would be attractive.
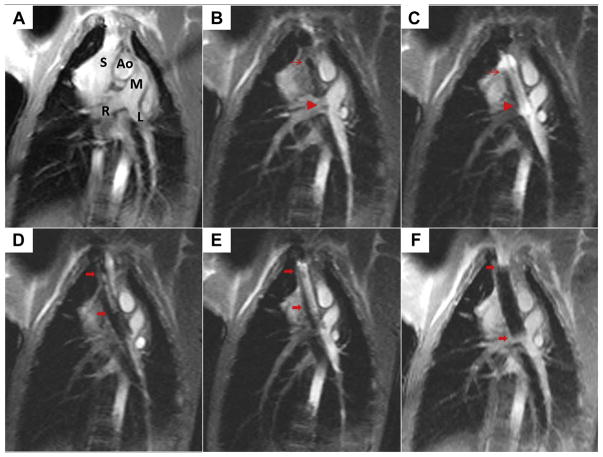
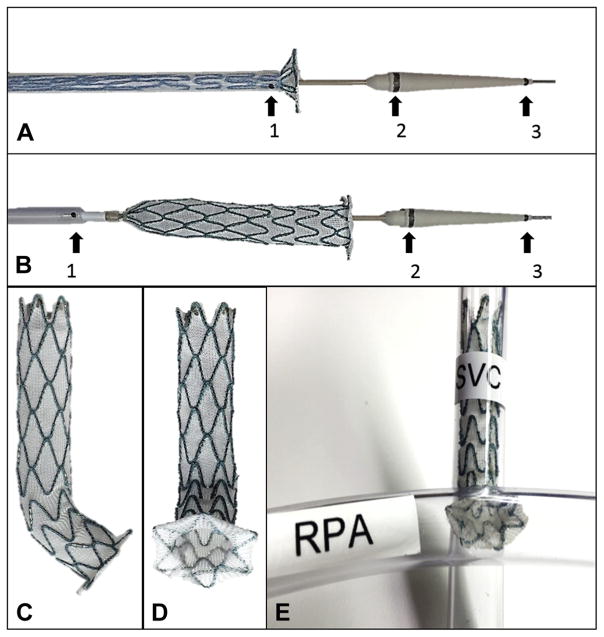
Methods: Fifteen naive swine underwent transcatheter cavopulmonary anastomosis and shunt creation under 1.5-T MRI guidance. An MRI antenna-needle was advanced from the superior vena cava into the target pulmonary artery bifurcation using real-time MRI guidance. In 10 animals, balloon-expanded off-the-shelf endografts secured a proximal end-to-end caval anastomosis and a distal end-to-side pulmonary anastomosis that preserved blood flow to both branch pulmonary arteries. In 5 animals, this was achieved with a novel, purpose-built, self-expanding device.
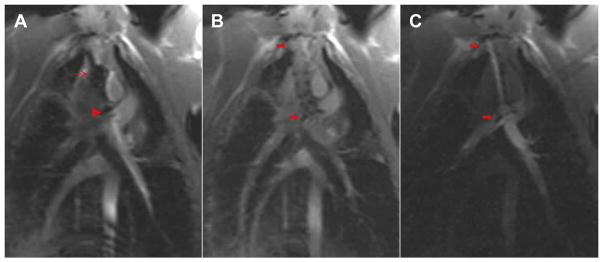
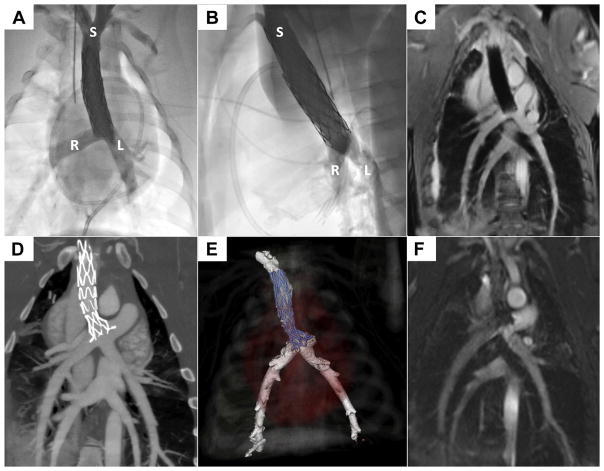
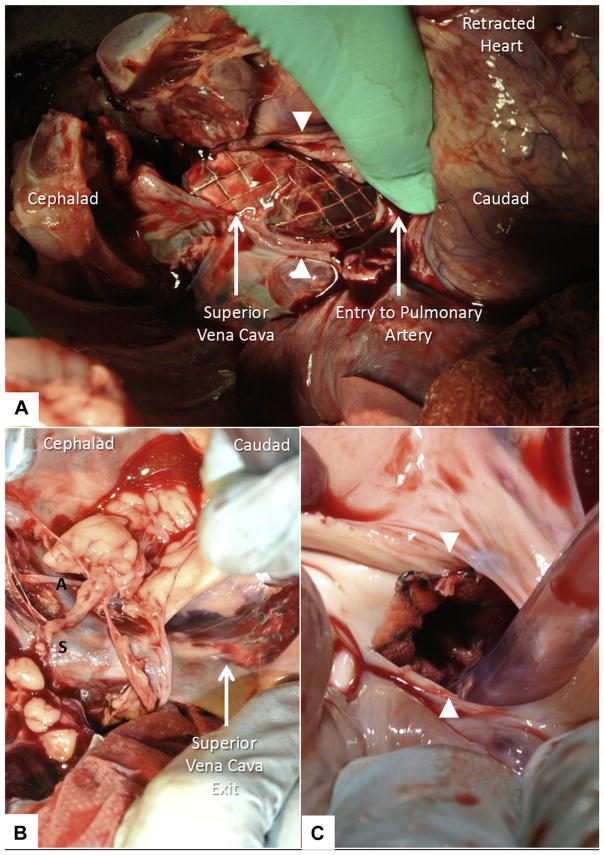
Results: Real-time MRI needle access of target vessels (pulmonary artery), endograft delivery, and superior vena cava shunt to pulmonary arteries were successful in all animals. All survived the procedure without complications. Intraprocedural real-time MRI, post-procedural MRI, x-ray angiography, computed tomography, and necropsy showed patent shunts with bidirectional pulmonary artery blood flow.
Conclusions: MRI guidance enabled a complex, closed-chest, beating-heart, pediatric, transcatheter structural heart procedure. In this study, MRI guided trajectory planning and reproducible, reliable bidirectional cavopulmonary shunt creation.
Keywords: congenital heart disease; image-guided intervention; interventional MRI; real-time MRI; sutureless anastomosis; vascular shunt.
Copyright © 2016 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Interventions in Complex Congenital Heart Disease: The Exciting Potential of Magnetic Resonance Imaging.JACC Cardiovasc Interv. 2016 May 9;9(9):971-2. doi: 10.1016/j.jcin.2016.03.009. Epub 2016 Apr 13. JACC Cardiovasc Interv. 2016. PMID: 27085577 No abstract available.
References
-
- Glenn WW. Circulatory bypass of the right side of the heart. IV. Shunt between superior vena cava and distal right pulmonary artery; report of clinical application. N Engl J Med. 1958;259:117–20. - PubMed
-
- Hopkins RA, Armstrong BE, Serwer GA, Peterson RJ, Oldham HN., Jr Physiological rationale for a bidirectional cavopulmonary shunt. A versatile complement to the Fontan principle. J Thorac Cardiovasc Surg. 1985;90:391–8. - PubMed
-
- Pandya B, Quail MA, Steeden JA, et al. Real-time magnetic resonance assessment of septal curvature accurately tracks acute hemodynamic changes in pediatric pulmonary hypertension. Circ Cardiovasc Imaging. 2014;7:706–13. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
