

Post traumatic deafness: a pictorial review of CT and MRI findings
- PMID: 27085885
- PMCID: PMC4877355
- DOI: 10.1007/s13244-016-0490-9
Post traumatic deafness: a pictorial review of CT and MRI findings
Abstract
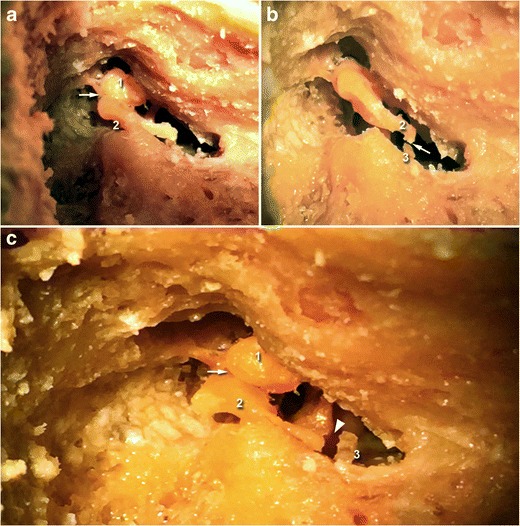
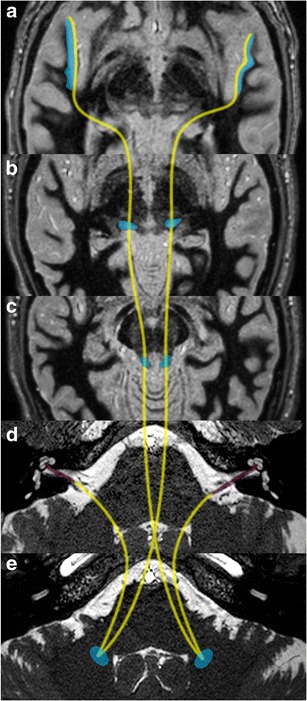
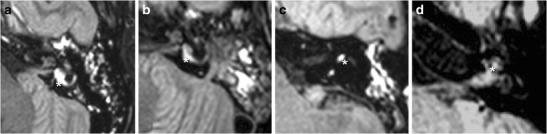
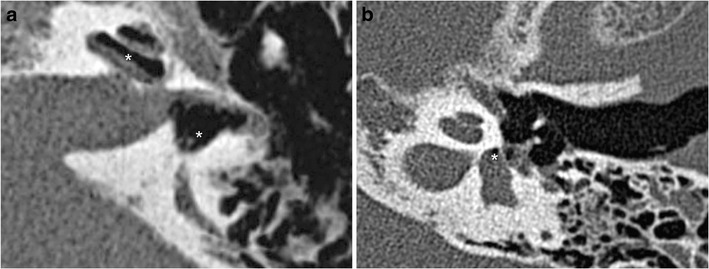
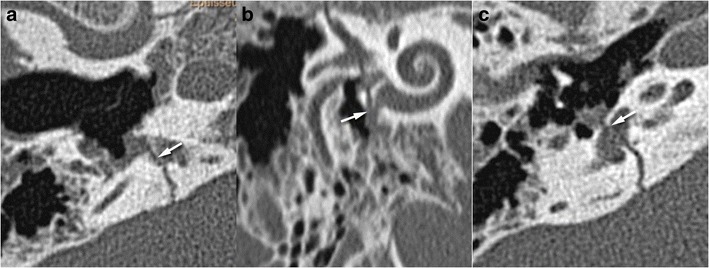
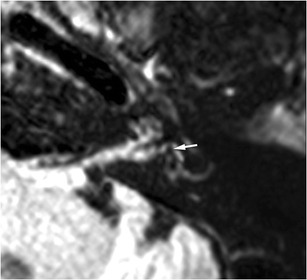
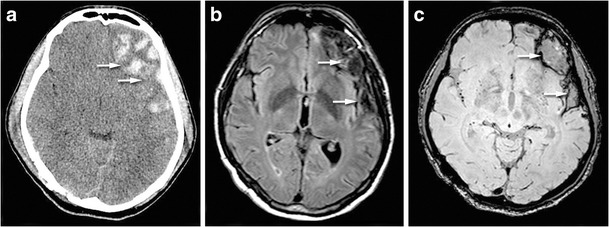
Hearing loss is a common functional disorder after trauma, and radiologists should be aware of the ossicular, labyrinthine or brain lesions that may be responsible. After a trauma, use of a systematic approach to explore the main functional components of auditory pathways is essential. Conductive hearing loss is caused by the disruption of the conductive chain, which may be due to ossicular luxation or fracture. This pictorial review firstly describes the normal 2-D and 3-D anatomy of the ossicular chain, including the incudo-malleolar and incudo-stapedial joints. The role of 3-D CT in the post-traumatic evaluation of injury to the temporal bone is then evaluated. In the case of sensorineural hearing loss, CT can detect pneumolabyrinth and signs of perilymphatic fistulae but fails to detect subtle lesions within the inner ear, such as labyrinthine haemorrhage or localized brain axonal damage along central auditory pathways. The role that MRI with 3-D-FLAIR acquisition plays in the detection of inner ear haemorrhage and post-traumatic lesions of the brain parenchyma that may lead to auditory agnosia is also discussed.
Key points: • The most common middle ear injuries are incudo-malleolar and incudo-stapedial joint luxation. • In patients with SNHL, CT can detect pneumolabyrinth or perilymphatic fistula • 3-D-FLAIR MRI appears the best sequence to highlight labyrinthine haemorrhage • Axonal damage and brain hematoma may lead to deafness.
Keywords: CT scan; Ear ossicles; Magnetic resonance imaging; Temporal bone deafness; Trauma.
Figures


References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
