

Recurrent Clostridium difficile infection associates with distinct bile acid and microbiome profiles
- PMID: 27086647
- PMCID: PMC5214573
- DOI: 10.1111/apt.13616
Recurrent Clostridium difficile infection associates with distinct bile acid and microbiome profiles
Abstract
Background: The healthy microbiome protects against the development of Clostridium difficile infection (CDI), which typically develops following antibiotics. The microbiome metabolises primary to secondary bile acids, a process if disrupted by antibiotics, may be critical for the initiation of CDI.
Aim: To assess the levels of primary and secondary bile acids associated with CDI and associated microbial changes.
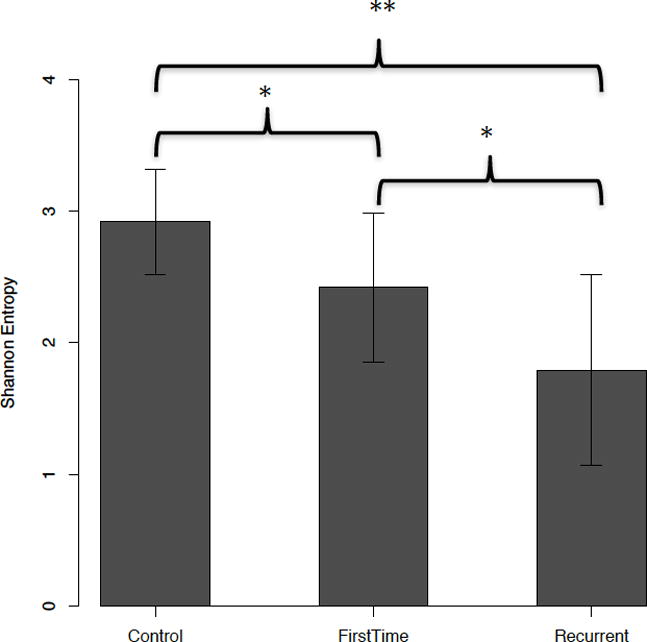
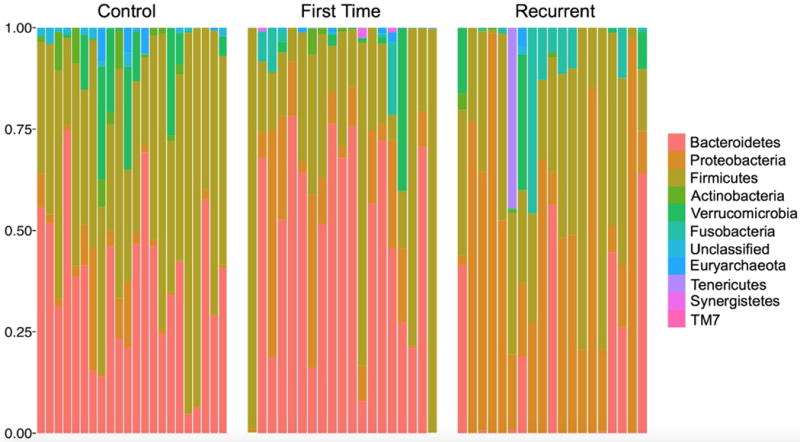
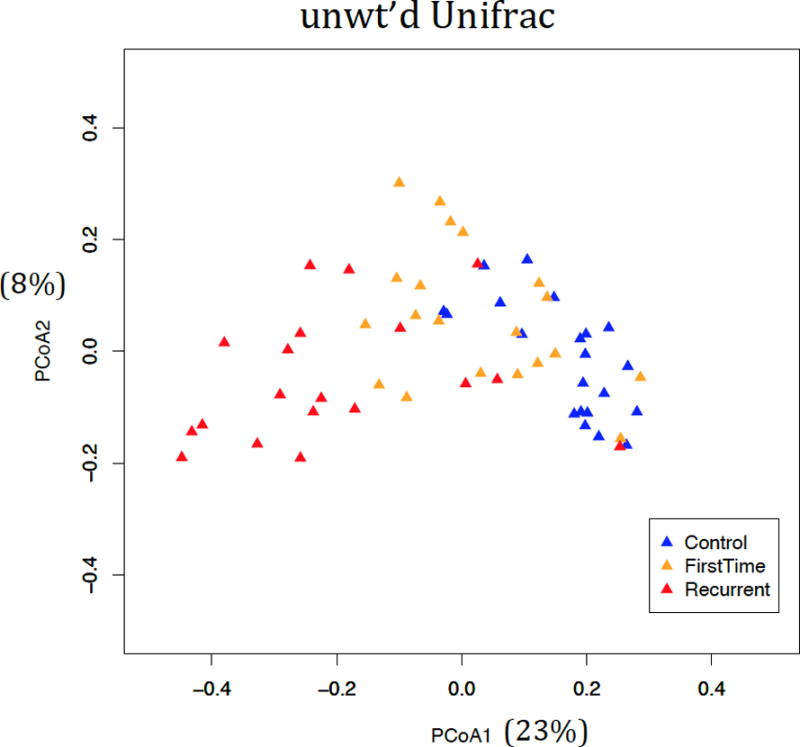
Methods: Stool and serum were collected from patients with (i) first CDI (fCDI), (ii) recurrent CDI (rCDI) and (iii) healthy controls. 16S rRNA sequencing and bile salt metabolomics were performed. Random forest regression models were constructed to predict disease status. PICRUSt analyses were used to test for associations between predicted bacterial bile salt hydrolase (BSH) gene abundances and bile acid levels.
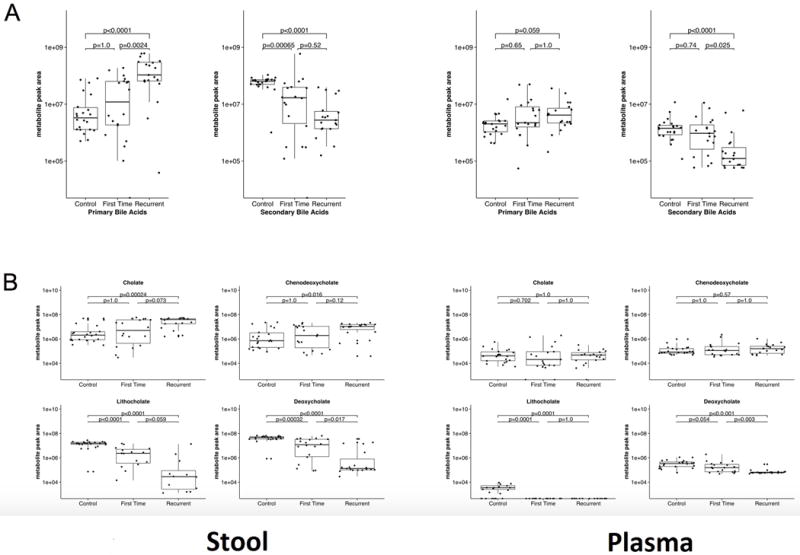
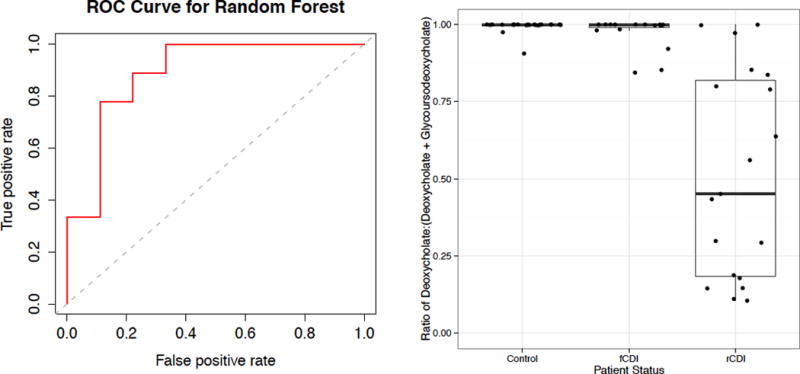
Results: Sixty patients (20 fCDI, 19 rCDI and 21 controls) were enrolled. Secondary bile acids in stool were significantly elevated in controls compared to rCDI and fCDI (P < 0.0001 and P = 0.0007 respectively). Primary bile acids in stool were significantly elevated in rCDI compared to controls (P < 0.0001) and in rCDI compared to fCDI (P = 0.02). Using random forest regression, we distinguished rCDI and fCDI patients 84.2% of the time using bile acid ratios. Stool deoxycholate to glycoursodeoxycholate ratio was the single best predictor. PICRUSt analyses found significant differences in predicted abundances of bacterial BSH genes in stool samples across the groups.
Conclusions: Primary and secondary bile acid composition in stool was different in those with rCDI, fCDI and controls. The ratio of stool deoxycholate to glycoursodeoxycholate was the single best predictor of disease state and may be a potential biomarker for recurrence.
© 2016 John Wiley & Sons Ltd.
Conflict of interest statement
Financial disclosures: no conflicts of interest to report for any authors in regards to the work presented in this manuscript.
Figures
References
-
- Bartlett JG. Narrative review: the new epidemic of Clostridium difficile-associated enteric disease. Ann Intern Med. 2006;145:758–764. - PubMed
-
- O’Connor JR, Johnson S, Gerding DN. Clostridium difficile infection caused by the epidemic BI/NAP1/027 strain. Gastroenterology. 2009;136:1913–1924. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources