

Vitamin D status in mothers with pre-eclampsia and their infants: a case-control study from Serbia, a country without a vitamin D fortification policy
- PMID: 27087002
- PMCID: PMC10261584
- DOI: 10.1017/S1368980016000409
Vitamin D status in mothers with pre-eclampsia and their infants: a case-control study from Serbia, a country without a vitamin D fortification policy
Abstract
Objective: The objective of the present study was to determine if vitamin D intake and status are associated with pre-eclampsia in a country without a vitamin D fortification policy.
Design: A case-control study of pregnancies with (case) and without (control) pre-eclampsia was conducted from January to April when UVB is minimal. Maternal and cord blood obtained at delivery were measured for plasma 25-hydroxycholecalciferol (25-OH-D3), 3-epimer of 25-OH-D3 (3-epi-25-OH-D3) and 24,25-dihydroxycholecalciferol (24,25-(OH)2D3) by LC-MS/MS and maternal 1,25-dihydroxyvitamin D (1,25-(OH)2D). Differences between groups were tested with ANOVA and Bonferroni post hoc tests (P<0·05).
Setting: Clinical Center of Serbia.
Subjects: Pregnant women with and without pre-eclampsia (n 60) and their infants.
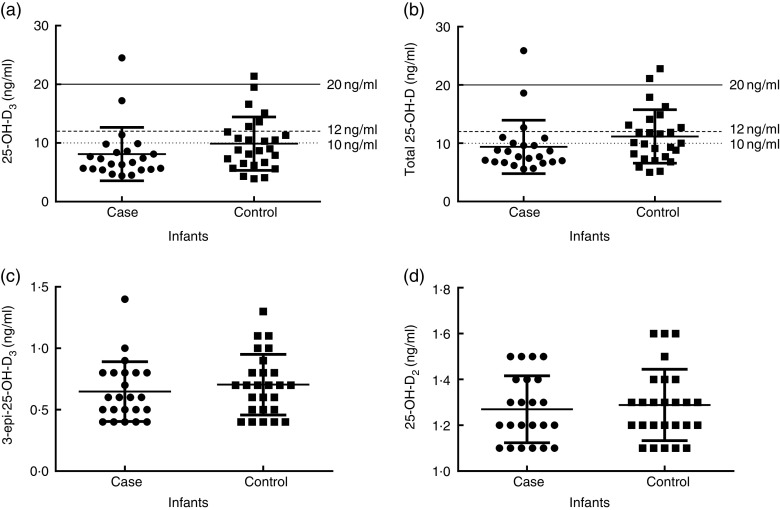
Results: Exogenous vitamin D intake (0·95-16·25 µg/d (38-650 IU/d)) was not significantly different between groups. Women with pre-eclampsia delivered infants at an earlier gestational age and had significantly lower mean total plasma 25-hydroxyvitamin D (25-OH-D; case: 11·2 (sd 5·1); control: 16·1 (sd 5·7) ng/ml; P=0·0006), 25-OH-D3 (case: 10·0 (sd 4·9); control: 14·2 (sd 5·8) ng/ml; P=0·002), 3-epi-25-OH-D3 (case: 0·5 (sd 0·2); control: 0·7 (sd 0·2) ng/ml; P=0·0007) and 1,25-(OH)2D (case: 56·5 (sd 26·6); control: 81·0 (sd 25·7) pg/ml; P=0·018), while 24,25-(OH)2D3 was not different between groups. Infants did not differ in total plasma 25-OH-D, 25-OH-D3, 3-epi-25-OH-D3 and 24,25-(OH)2D3, but the mean proportion of 3-epi-25-OH-D3 was higher in the infant case group (case: 7·9 (sd 1·1); control: 7·0 (sd 1·4) % of total 25-OH-D3; P=0·005).
Conclusions: A high prevalence of vitamin D deficiency, as defined by plasma 25-OH-D<12 ng/ml, was observed in 47 % of all mothers and 77 % of all infants. These data underscore the need for prenatal vitamin D supplementation and a food fortification policy in Serbia.
Keywords: C3-epi-25-hydroxycholecalciferol; LC–MS/MS; Maternal and cord blood; Pre-clampsia; Pregnancy; Vitamin D status.
Figures

Similar articles
-
Plasma 3-Epi-25-Hydroxycholecalciferol Can Alter the Assessment of Vitamin D Status Using the Current Reference Ranges for Pregnant Women and Their Newborns.J Nutr. 2016 Jan;146(1):70-5. doi: 10.3945/jn.115.220095. Epub 2015 Nov 25. J Nutr. 2016. PMID: 26609169
-
Vitamin D status is associated with uteroplacental dysfunction indicated by pre-eclampsia and small-for-gestational-age birth in a large prospective pregnancy cohort in Ireland with low vitamin D status.Am J Clin Nutr. 2016 Aug;104(2):354-61. doi: 10.3945/ajcn.116.130419. Epub 2016 Jun 29. Am J Clin Nutr. 2016. PMID: 27357092
-
Maternal-fetal-infant dynamics of the C3-epimer of 25-hydroxyvitamin D.Clin Biochem. 2014 Jun;47(9):816-22. doi: 10.1016/j.clinbiochem.2014.01.015. Epub 2014 Jan 22. Clin Biochem. 2014. PMID: 24462965
-
Iatrogenic vitamin D toxicity in an infant--a case report and review of literature.J Steroid Biochem Mol Biol. 2015 Apr;148:14-8. doi: 10.1016/j.jsbmb.2015.01.022. Epub 2015 Jan 27. J Steroid Biochem Mol Biol. 2015. PMID: 25636720 Review.
-
25(OH)D3-enriched or fortified foods are more efficient at tackling inadequate vitamin D status than vitamin D3.Proc Nutr Soc. 2018 Aug;77(3):282-291. doi: 10.1017/S0029665117004062. Epub 2017 Nov 27. Proc Nutr Soc. 2018. PMID: 29173203 Free PMC article. Review.
Cited by
-
C3-Epimer of 25-Hydroxyvitamin D3 as a Superior Marker for Predicting the Severity of Chronic Kidney Disease in Rheumatoid Arthritis Patients.Oxid Med Cell Longev. 2022 Apr 22;2022:5268706. doi: 10.1155/2022/5268706. eCollection 2022. Oxid Med Cell Longev. 2022. PMID: 35498132 Free PMC article.
-
Antenatal Exposure to UV-B Radiation and Preeclampsia: A Retrospective Cohort Study.J Am Heart Assoc. 2021 Jul 6;10(13):e020246. doi: 10.1161/JAHA.120.020246. Epub 2021 Jun 22. J Am Heart Assoc. 2021. PMID: 34155917 Free PMC article.
-
Maternal Circulating Vitamin D Level, Targeted Supplementation, and Perinatal Outcomes in Twin Pregnancy.Nutrients. 2024 Jul 12;16(14):2239. doi: 10.3390/nu16142239. Nutrients. 2024. PMID: 39064682 Free PMC article.
-
Vitamin D research and public health nutrition: a current perspective.Public Health Nutr. 2017 Jul;20(10):1713-1717. doi: 10.1017/S1368980017001835. Public Health Nutr. 2017. PMID: 29125453 Free PMC article. No abstract available.
-
Serum and urine vitamin D metabolite analysis in early preeclampsia.Endocr Connect. 2018 Jan;7(1):199-210. doi: 10.1530/EC-17-0308. Epub 2017 Dec 7. Endocr Connect. 2018. PMID: 29217650 Free PMC article.
References
-
- Steegers EA, von Dadelszen P, Duvekot JJ et al.. (2010) Pre-eclampsia. Lancet 376, 631–644. - PubMed
-
- Haugen M, Brantsaeter AL, Trogstad L et al.. (2009) Vitamin D supplementation and reduced risk of preeclampsia in nulliparous women. Epidemiology 20, 720–726. - PubMed
-
- Tabesh M, Salehi-Abargouei A, Tabesh M et al.. (2013) Maternal vitamin D status and risk of pre-eclampsia: a systematic review and meta-analysis. J Clin Endocrinol Metab 98, 3165–3173. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
