

Fluid therapy in the perioperative setting-a clinical review
- PMID: 27087980
- PMCID: PMC4833950
- DOI: 10.1186/s40560-016-0154-3
Fluid therapy in the perioperative setting-a clinical review
Abstract
Background: Perioperative hypovolemia and fluid overload have effects on both complications following surgery and on patient survival. Therefore, the administration of intravenous fluids before, during, and after surgery at the right time and in the right amounts is of great importance. This review aims to analyze the literature concerning perioperative fluid therapy in abdominal surgery and to provide evidence-based recommendations for clinical practice.
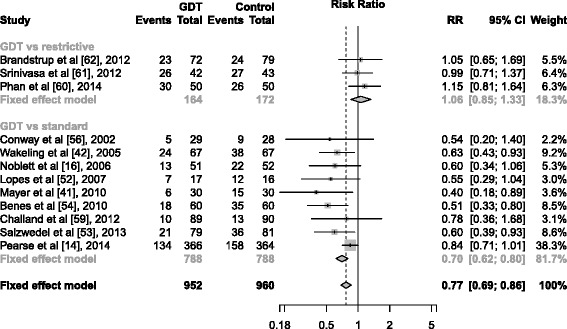
Results: Preoperative oral or intravenous administration of carbohydrate containing fluids has been shown to improve postoperative well-being and muscular strength and to reduce insulin resistance. Hence, the intake of fluid (preferably containing carbohydrates) should be encouraged up to 2 h prior to surgery in order to avoid dehydration. Excessive intravenous fluid administration adds to tissue inflammation and edema formation, thereby compromising tissue healing. During major abdominal surgery a "zero-balance" intraoperative fluid strategy aims at avoiding fluid overload (and comparable to the so-called restrictive approach) as well as goal-directed fluid therapy (GDT). Both proved to significantly reduce postoperative complications when compared to "standard fluid therapy". Trials comparing "restrictive" or zero-balance and GDT have shown equal results, as long as fluid overload is avoided in the GDT group as well (categorized as "zero-balance GDT"). It is possible that high-risk surgical patients, such as those undergoing acute surgery, may benefit from the continuous monitoring of circulatory status that the GDT provides. Data on this group of patients is not available at present, but trials are ongoing.
Conclusion: In elective surgery, the zero-balance approach has shown to reduce postoperative complications and is easily applied for most patients. It is less expensive and simpler than the zero-balance GDT approach and therefore recommended in this review. In outpatient surgery, 1-2 L of balanced crystalloids reduces postoperative nausea and vomiting and improves well-being.
Keywords: Fluid therapy; Goal-directed fluid therapy; Outcome of surgery; Postoperative complications; Restricted; Third space; Third space loss.
Figures
References
-
- Brandstrup B, Tønnesen H, Beier-Holgersen R, et al. Effects of intravenous fluid restriction on postoperative complications: comparison of two perioperative fluid regimens: a randomized assessor-blinded multicenter trial. Ann Surg. 2003;238(5):641–8. doi: 10.1097/01.sla.0000094387.50865.23. - DOI - PMC - PubMed
-
- Kulemann B, Timme S, Seifert G, et al. Intraoperative crystalloid overload leads to substantial inflammatory infiltration of intestinal anastomoses—a histomorphological analysis. Surg (United States) 2013;154(3):596–603. - PubMed
-
- Wuethrich PY, Burkhard FC, Thalmann GN, Stueber F, Studer UE. Restrictive deferred hydration combined with preemptive norepinephrine infusion during radical cystectomy reduces postoperative complications and hospitalization time. Anesthesiology. 2014;120(2):365–77. doi: 10.1097/ALN.0b013e3182a44440. - DOI - PubMed
-
- Neal JM, Wilcox RT, Allen HW, Low DE. Near-total esophagectomy: the influence of standardized multimodal management and intraoperative fluid restriction. Reg Anesth Pain Med. 2003;28(4):328–34. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
