

Association of Antenatal Corticosteroids With Mortality, Morbidity, and Neurodevelopmental Outcomes in Extremely Preterm Multiple Gestation Infants
- PMID: 27088897
- PMCID: PMC5270648
- DOI: 10.1001/jamapediatrics.2016.0104
Association of Antenatal Corticosteroids With Mortality, Morbidity, and Neurodevelopmental Outcomes in Extremely Preterm Multiple Gestation Infants
Abstract
Importance: Little is known about the effects of antenatal corticosteroids (ANS) on extremely preterm multiples.
Objective: To examine if use of ANS is associated with improvement in major outcomes in extremely preterm multiples.
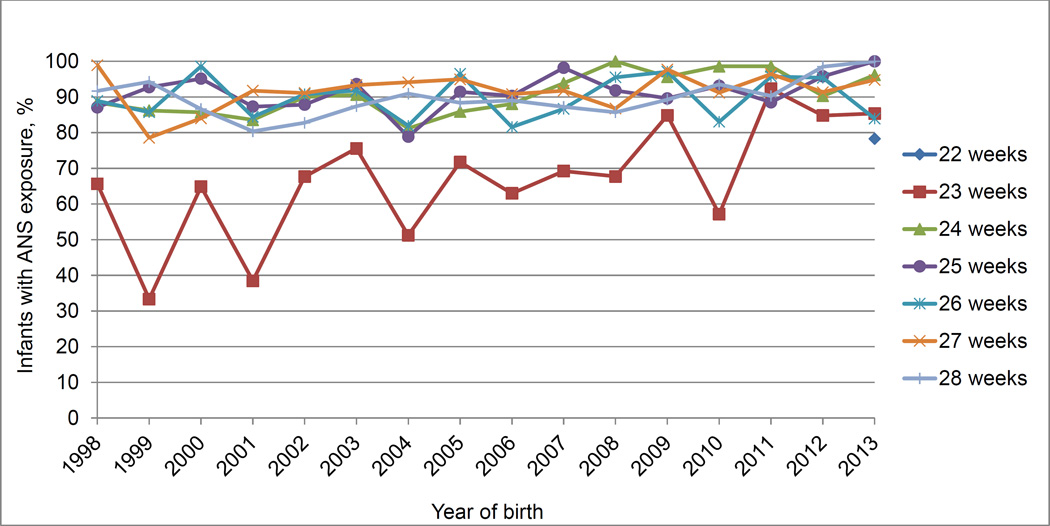
Design, setting, and participants: Infants with a gestational age between 22 and 28 weeks born at a National Institute of Child Health and Human Development Neonatal Research Network center were studied between January 1998 and December 2013. Generalized estimating equation models were used to generate adjusted relative risks (aRR) controlling for important maternal and neonatal variables.
Exposure: Antenatal corticosteroids.
Main outcomes and measures: In-hospital mortality and the composite outcome of neurodevelopmental impairment at 18 to 22 months' corrected age or death before assessment.
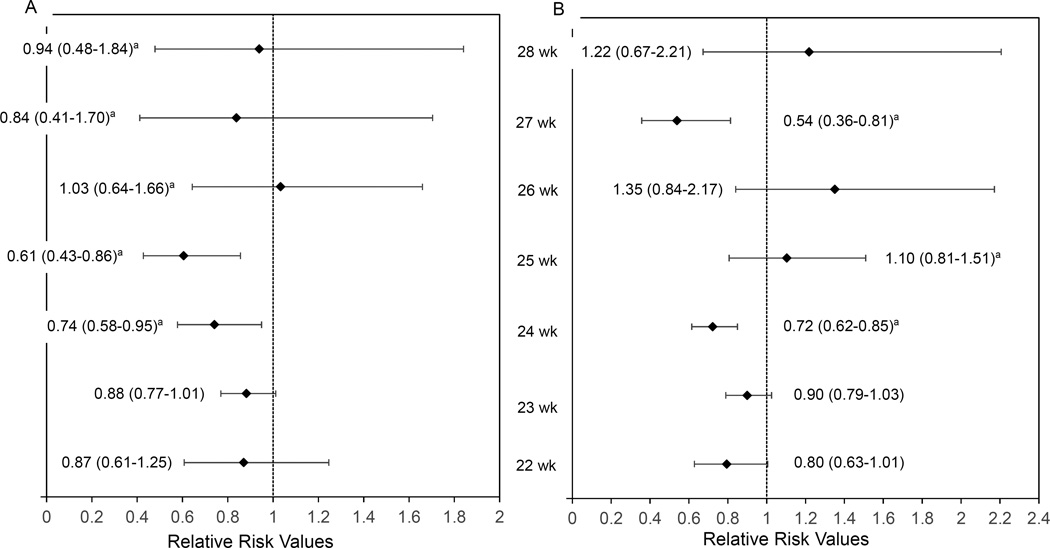
Results: A total of 6925 multiple-birth infants were studied; 5775 of 6925 (83.4%) were twins, and 4276 (61.7%) were white. Of the total study population, 6094 (88%) were born to women who received ANS. In-hospital mortality was lower among infants with exposure to ANS vs no exposure (aRR = 0.87; 95% CI, 0.78-0.96). Neurodevelopmental impairment or death was not significantly lower among those exposed to ANS vs no exposure (aRR = 0.93; 95% CI, 0.84-1.03). Other adverse outcomes that occurred less frequently among infants of women receiving ANS included severe intraventricular hemorrhage (aRR = 0.68; 95% CI, 0.58-0.78) and the combined outcomes of necrotizing enterocolitis or death and severe intraventricular hemorrhage or death. Subgroup analyses indicated that exposure to ANS was associated with a lower risk of mortality and a lower composite of neurodevelopmental impairment or mortality among nonsmall for gestational age multiples (aRR = 0.82; 95% CI, 0.74-0.92; and aRR = 0.89; 95% CI, 0.80-0.98, respectively) and a higher risk among small for gestational age multiples (aRR = 1.40; 95% CI, 1.02-1.93; and aRR = 1.62; 95% CI, 1.22-2.16, respectively). Antenatal corticosteroids were associated with higher neurodevelopmental impairment or mortality among multiple-birth infants of mothers with diabetes (aRR = 1.55; 95% CI, 1.00-2.38) but not among infants of mothers without diabetes (aRR = 0.91; 95% CI, 0.83-1.01).
Conclusions and relevance: Compared with no exposure, exposure to ANS was associated with a lower risk of mortality in extremely preterm multiples, with no significant differences in the composite of neurodevelopmental impairment or death. Future research should investigate the increased risks of mortality and the composite of neurodevelopmental impairment or death associated with exposure to corticosteroids among small for gestational age multiples.
Conflict of interest statement
Disclosures: All authors have no conflicts of interest and no financial relationships relevant to this article to disclose.
Figures
References
-
- Warner BB, Kiely JL, Donovan EF. Multiple births and outcome. Clin Perinatol. 2000;27(2):347–361. - PubMed
-
- Roberts D, Dalziel S. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev. 2006:CD004454. - PubMed
-
- Gilstrap LC, Christensen R, Clewell WH, et al. Effect of corticosteroids for fetal maturation on perinatal outcomes. NIH Consensus Development Panel on the Effect of Corticosteroids for Fetal Maturation on Perinatal Outcomes. JAMA. 1995;273(5):413–418. - PubMed
-
- Papile LA, Burstein J, Burstein R, Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J Pediatr. 1978;92(4):529–534. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U10 HD027856/HD/NICHD NIH HHS/United States
- U10 HD021373/HD/NICHD NIH HHS/United States
- U10 HD021385/HD/NICHD NIH HHS/United States
- UG1 HD087226/HD/NICHD NIH HHS/United States
- UG1 HD027853/HD/NICHD NIH HHS/United States
- U10 HD053109/HD/NICHD NIH HHS/United States
- U10 HD027904/HD/NICHD NIH HHS/United States
- UG1 HD027856/HD/NICHD NIH HHS/United States
- UG1 HD034216/HD/NICHD NIH HHS/United States
- UG1 HD027904/HD/NICHD NIH HHS/United States
- UG1 HD021385/HD/NICHD NIH HHS/United States
- UG1 HD027880/HD/NICHD NIH HHS/United States
- UG1 HD053109/HD/NICHD NIH HHS/United States
- U10 HD034216/HD/NICHD NIH HHS/United States
- U10 HD036790/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
