

Human induced pluripotent stem cell-derived cardiomyocytes recapitulate the predilection of breast cancer patients to doxorubicin-induced cardiotoxicity
- PMID: 27089514
- PMCID: PMC5086256
- DOI: 10.1038/nm.4087
Human induced pluripotent stem cell-derived cardiomyocytes recapitulate the predilection of breast cancer patients to doxorubicin-induced cardiotoxicity
Abstract
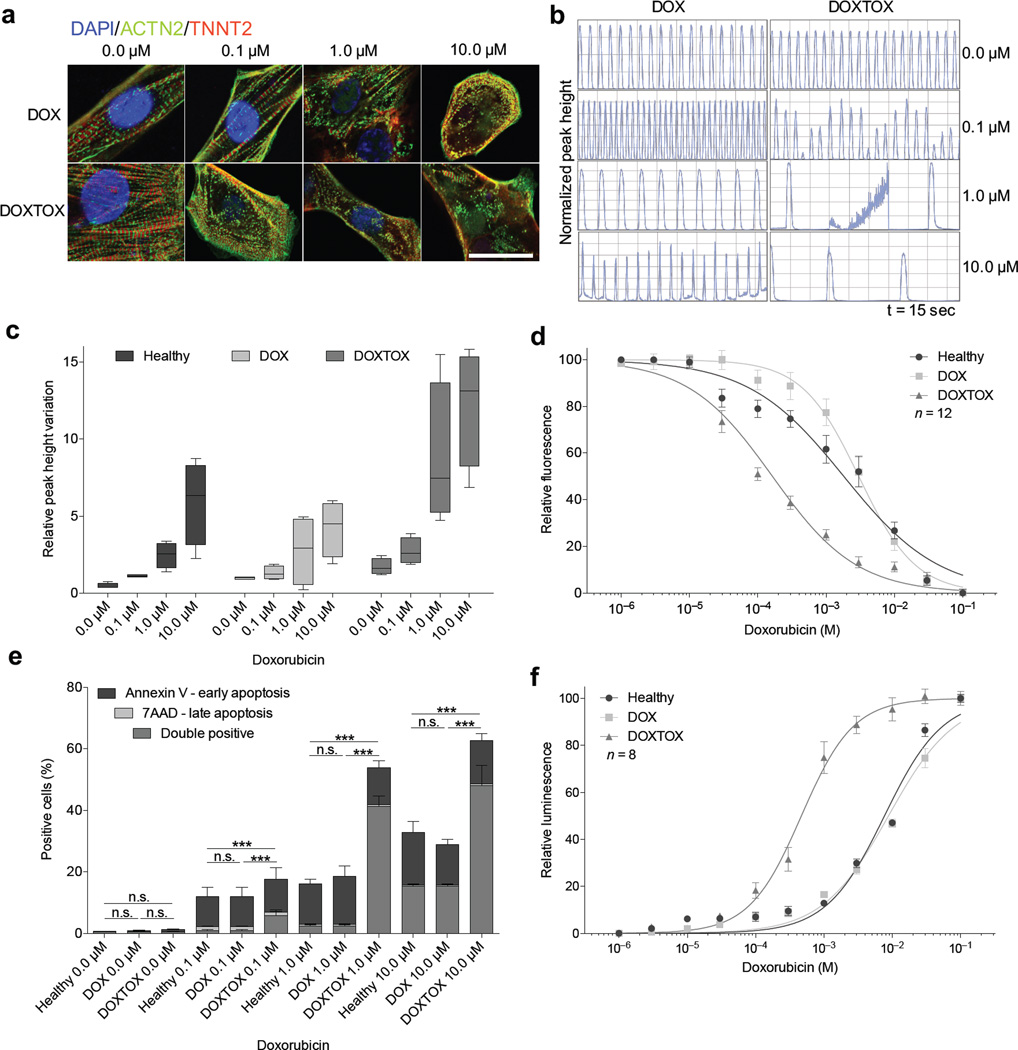
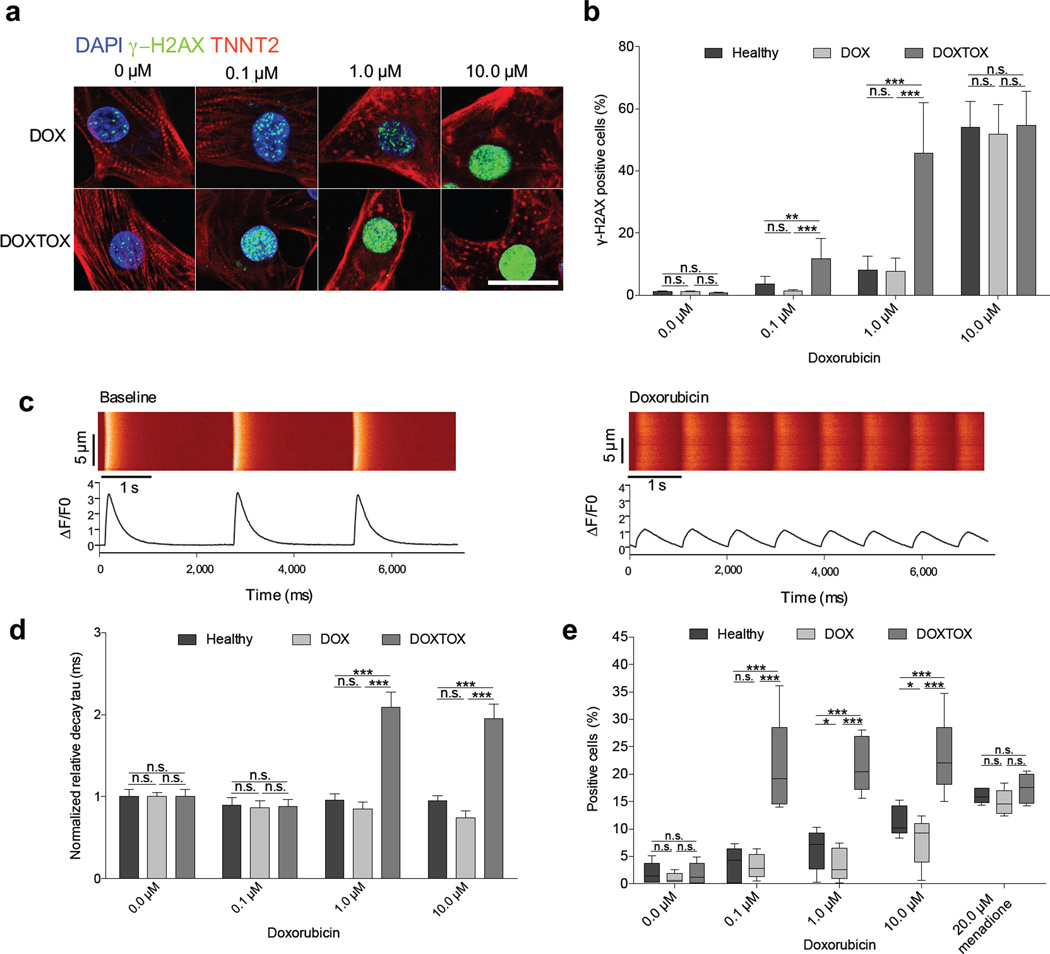
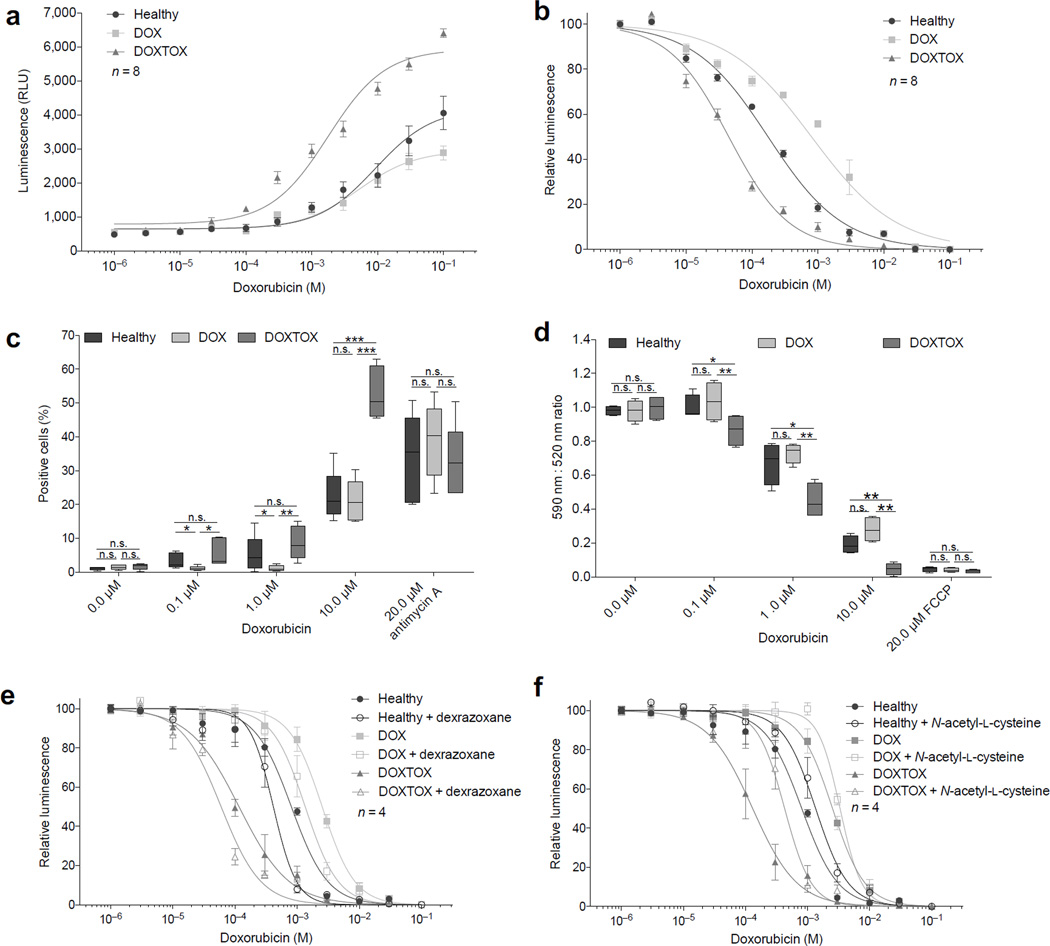
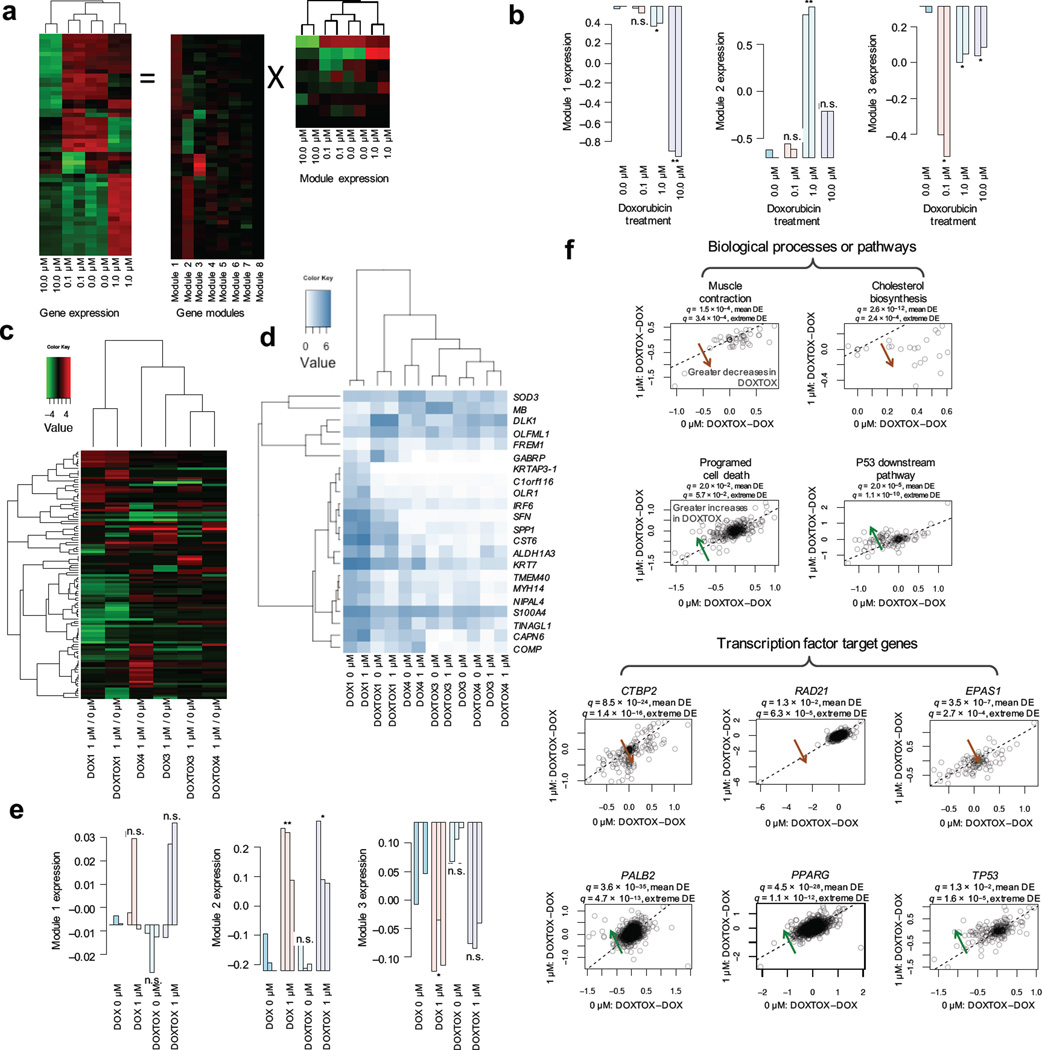
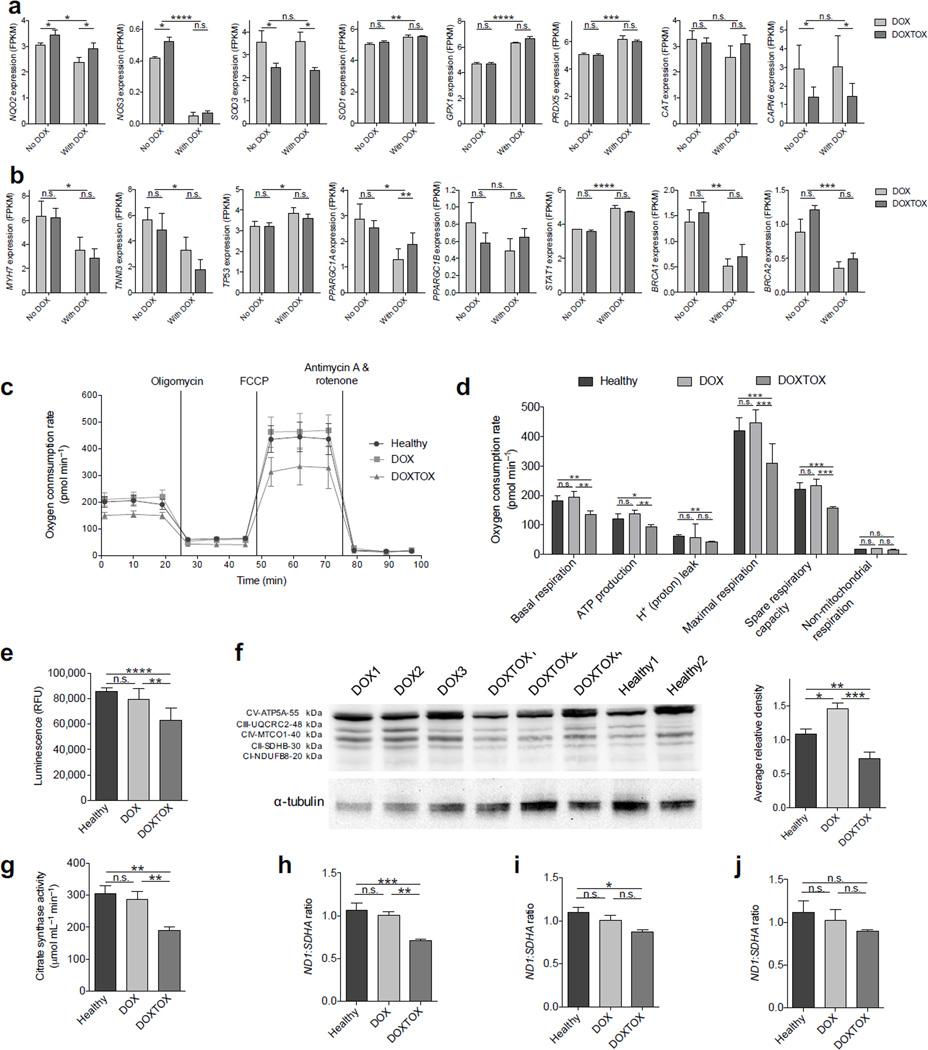
Doxorubicin is an anthracycline chemotherapy agent effective in treating a wide range of malignancies, but it causes a dose-related cardiotoxicity that can lead to heart failure in a subset of patients. At present, it is not possible to predict which patients will be affected by doxorubicin-induced cardiotoxicity (DIC). Here we demonstrate that patient-specific human induced pluripotent stem cell-derived cardiomyocytes (hiPSC-CMs) can recapitulate the predilection to DIC of individual patients at the cellular level. hiPSC-CMs derived from individuals with breast cancer who experienced DIC were consistently more sensitive to doxorubicin toxicity than hiPSC-CMs from patients who did not experience DIC, with decreased cell viability, impaired mitochondrial and metabolic function, impaired calcium handling, decreased antioxidant pathway activity, and increased reactive oxygen species production. Taken together, our data indicate that hiPSC-CMs are a suitable platform to identify and characterize the genetic basis and molecular mechanisms of DIC.
Figures

Comment in
-
Cardiotoxicity in a dish: new insights for personalized therapy.Nat Med. 2016 May 5;22(5):459-60. doi: 10.1038/nm.4095. Nat Med. 2016. PMID: 27149216 No abstract available.
References
-
- Lefrak EA, Pitha J, Rosenheim S, Gottlieb JA. A clinicopathologic analysis of adriamycin cardiotoxicity. Cancer. 1973;32:302–314. - PubMed
-
- Hoff, Von DD, et al. Risk factors for doxorubicin-induced congestive heart failure. Ann. Intern. Med. 1979;91:710–717. - PubMed
-
- Swain SM, Whaley FS, Ewer MS. Congestive heart failure in patients treated with doxorubicin: a retrospective analysis of three trials. Cancer. 2003;97:2869–2879. - PubMed
ONLINE REFERENCES
Publication types
MeSH terms
Substances
Grants and funding
- R24 GM061374/GM/NIGMS NIH HHS/United States
- R01 NS089533/NS/NINDS NIH HHS/United States
- R01 HL130020/HL/NHLBI NIH HHS/United States
- R01 LM005652/LM/NLM NIH HHS/United States
- R21 AG044815/AG/NIA NIH HHS/United States
- R01 HL123968/HL/NHLBI NIH HHS/United States
- R01 HL128170/HL/NHLBI NIH HHS/United States
- R01 AG020961/AG/NIA NIH HHS/United States
- K99 HL121177/HL/NHLBI NIH HHS/United States
- U01 GM061374/GM/NIGMS NIH HHS/United States
- T32 HL094274/HL/NHLBI NIH HHS/United States
- R01 GM102365/GM/NIGMS NIH HHS/United States
- R21 HL123655/HL/NHLBI NIH HHS/United States
- R00 HL121177/HL/NHLBI NIH HHS/United States
- R01 HL126527/HL/NHLBI NIH HHS/United States
- P30 CA124435/CA/NCI NIH HHS/United States
- R01 AR063963/AR/NIAMS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
