

White matter injury in ischemic stroke
- PMID: 27090751
- PMCID: PMC5677601
- DOI: 10.1016/j.pneurobio.2016.04.005
White matter injury in ischemic stroke
Abstract
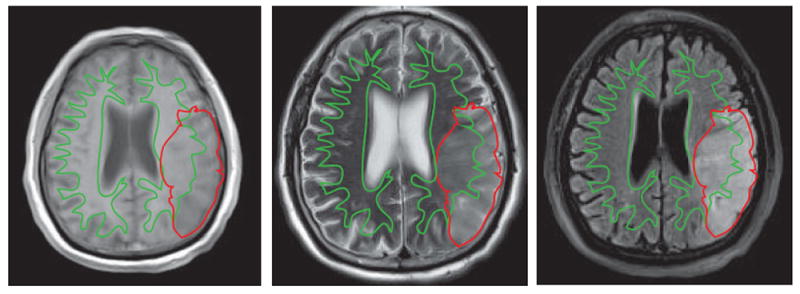
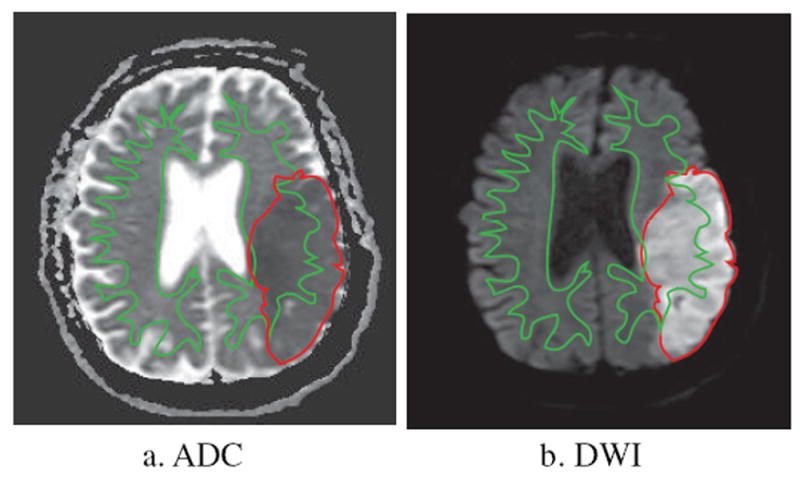
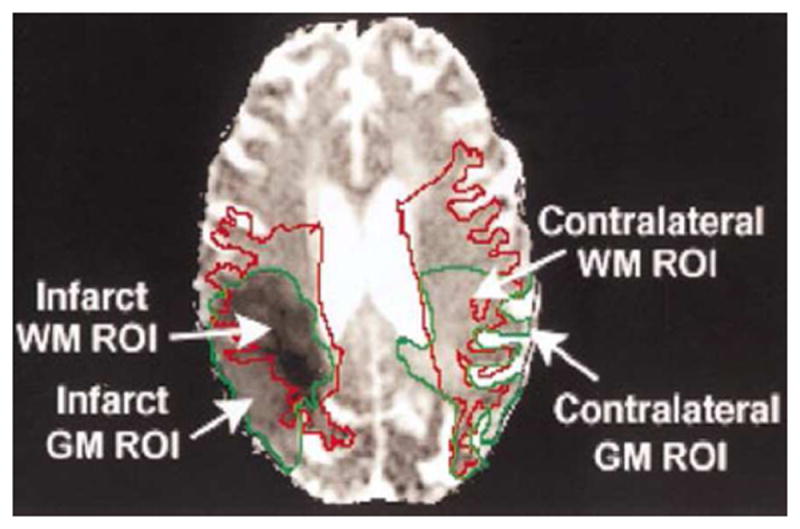
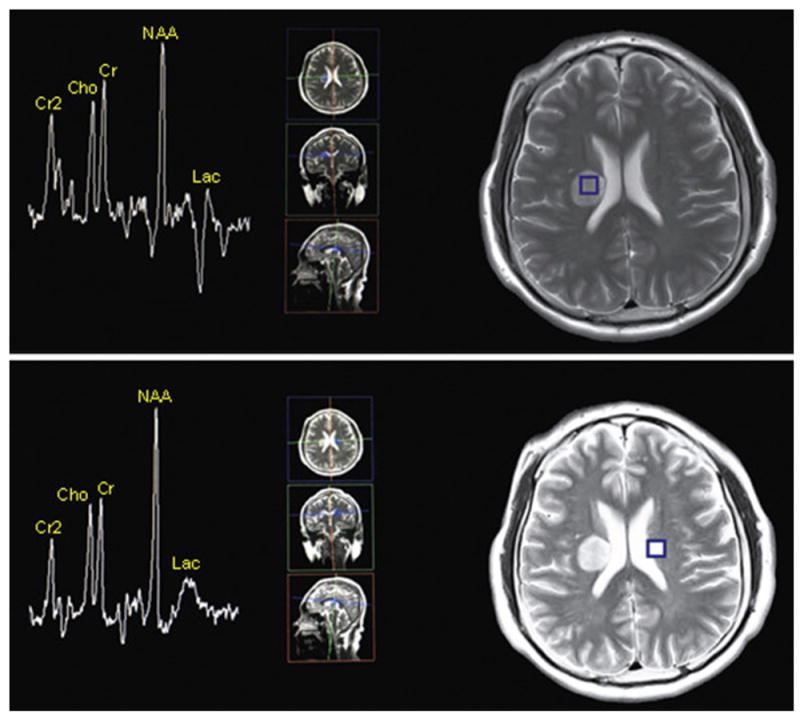
Stroke is one of the major causes of disability and mortality worldwide. It is well known that ischemic stroke can cause gray matter injury. However, stroke also elicits profound white matter injury, a risk factor for higher stroke incidence and poor neurological outcomes. The majority of damage caused by stroke is located in subcortical regions and, remarkably, white matter occupies nearly half of the average infarct volume. Indeed, white matter is exquisitely vulnerable to ischemia and is often injured more severely than gray matter. Clinical symptoms related to white matter injury include cognitive dysfunction, emotional disorders, sensorimotor impairments, as well as urinary incontinence and pain, all of which are closely associated with destruction and remodeling of white matter connectivity. White matter injury can be noninvasively detected by MRI, which provides a three-dimensional assessment of its morphology, metabolism, and function. There is an urgent need for novel white matter therapies, as currently available strategies are limited to preclinical animal studies. Optimal protection against ischemic stroke will need to encompass the fortification of both gray and white matter. In this review, we discuss white matter injury after ischemic stroke, focusing on clinical features and tools, such as imaging, manifestation, and potential treatments. We also briefly discuss the pathophysiology of WMI and future research directions.
Keywords: Axonal damage; Demyelination; Ischemic stroke; MRI; Oligodendrogenesis; Therapy; White matter injury.
Published by Elsevier Ltd.
Conflict of interest statement
All authors have no actual or potential conflicts of interest, including any financial, personal or other relationships with other people or organizations within three years of beginning of the submitted work.
Figures
References
-
- Alix JJ, Fern R. Glutamate receptor-mediated ischemic injury of premyelinated central axons. Annals of neurology. 2009;66:682–693. - PubMed
-
- Amaro S, Llull L, Renu A, Laredo C, Perez B, Vila E, Torres F, Planas AM, Chamorro A. Uric acid improves glucose-driven oxidative stress in human ischemic stroke. Annals of neurology. 2015;77:775–783. - PubMed
-
- Amiri-Nikpour MR, Nazarbaghi S, Hamdi-Holasou M, Rezaei Y. An open-label evaluator-blinded clinical study of minocycline neuroprotection in ischemic stroke: gender-dependent effect. Acta neurologica Scandinavica. 2015;131:45–50. - PubMed
-
- Axer H, Keyserlingk DG. Mapping of fiber orientation in human internal capsule by means of polarized light and confocal scanning laser microscopy. Journal of neuroscience methods. 2000;94:165–175. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
