

Myeloid malignancies in the real-world: Occurrence, progression and survival in the UK's population-based Haematological Malignancy Research Network 2004-15
- PMID: 27090942
- PMCID: PMC4911595
- DOI: 10.1016/j.canep.2016.03.011
Myeloid malignancies in the real-world: Occurrence, progression and survival in the UK's population-based Haematological Malignancy Research Network 2004-15
Abstract
Background: Population-based information on cancer incidence, prevalence and outcome are required to inform clinical practice and research; but contemporary data are lacking for many myeloid malignancy subtypes.
Methods: Set within a socio-demographically representative UK population of ∼4 million, myeloid malignancy data (N=5231 diagnoses) are from an established patient cohort. Information on incidence, survival (relative & overall), transformation/progression, and prevalence is presented for >20 subtypes.
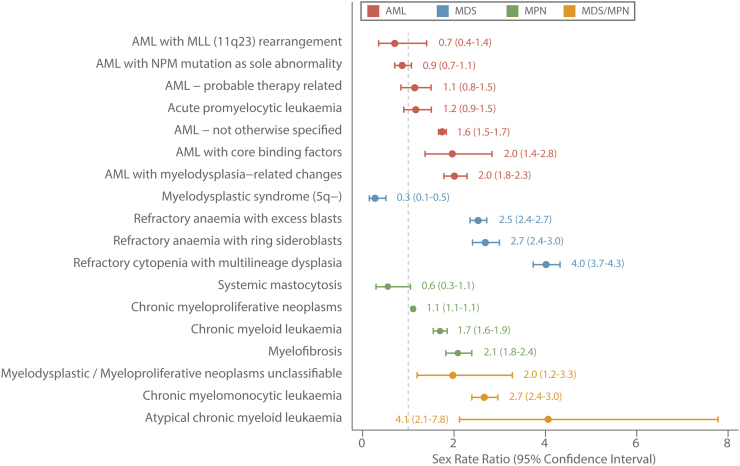
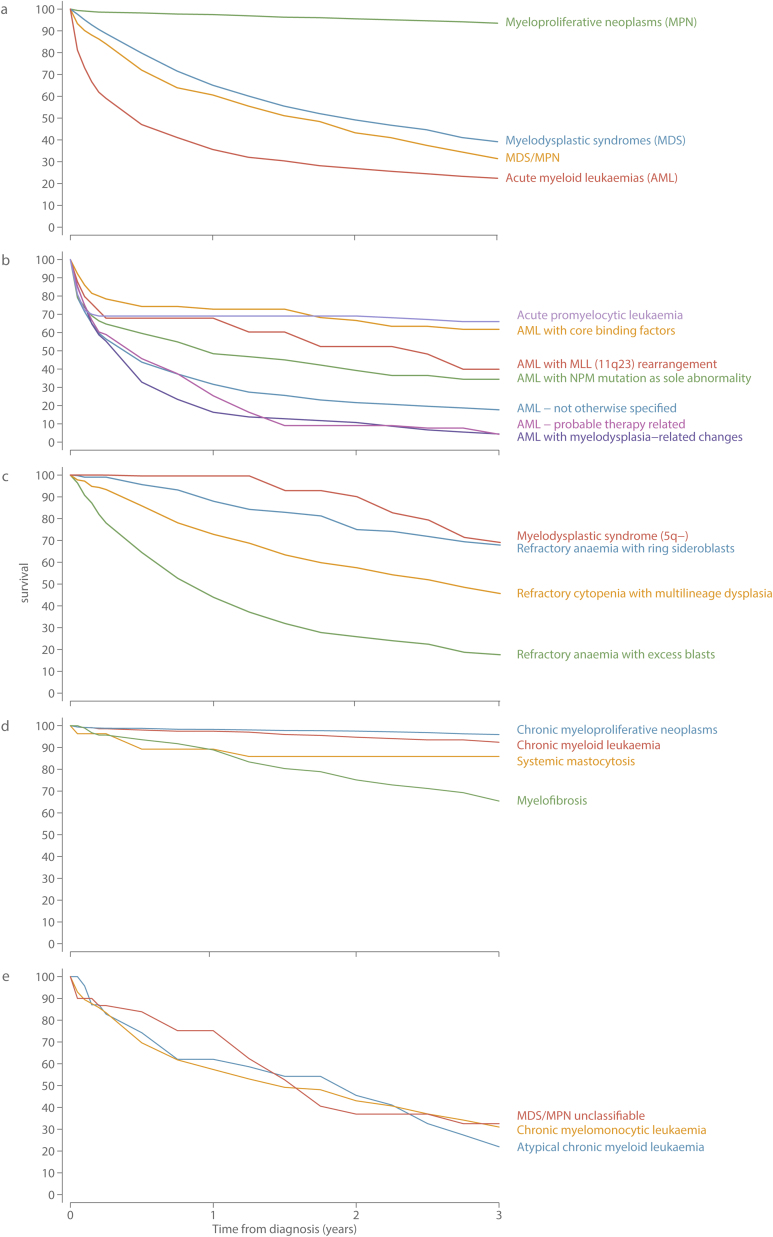
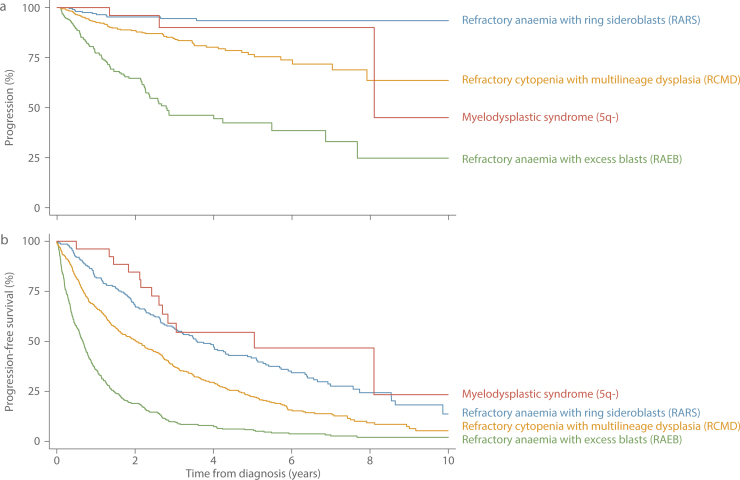
Results: The median diagnostic age was 72.4years (InterQuartile Range 61.6-80.2), but there was considerable subtype heterogeneity, particularly among the acute myeloid leukaemias (AML) where medians ranged from 20.3 (IQR 13.9-43.8) for AML 11q23 through to 73.7 (IQR 57.3-79.1) for AML with no recurrent genetic changes. Five-year Relative Survival (RS) estimates varied hugely; from <5% for aggressive entities like therapy-related AML (2.6%, 95% Confidence Interval 0.4-9.0) to >85% for indolent/treatable conditions like chronic myeloid leukaemia (89.8%, 95% CI 84.0-93.6). With a couple of notable exceptions, males experienced higher rates and worse survival than females: the age-standardized incidence rates of several conditions was 2-4 higher in males than females, and the 5-year RS for all subtypes combined was 48.8% (95% CI 46.5-51.2) and 60.4% (95% CI 57.7-62.9) for males and females respectively. During follow-up (potential minimum 2 years and maximum 11years) myelodysplastic syndrome (MDS) progression to AML ranged from 25% for refractory anaemia with excess blasts through to 5% for refractory anaemia with ring sideroblasts: the median interval between MDS and AML diagnosis was 9.0 months (IQR 4.8-17.4months).
Conclusions: The marked incidence and outcome variations seen by subtype, sex and age, confirm the requirement for "real-world" longitudinal data to inform aetiological hypotheses, healthcare planning, and future monitoring of therapeutic change. Several challenges for routine cancer registration were identified, including the need to link more effectively to diagnostic and clinical data sources, and to review policies on the recording of progressions and transformations.
Keywords: Acute myeloid leukaemia; Essential thrombocythaemia; Myelodysplastic syndromes; Myeloproliferative neoplasms; Polycythaemia vera.
Copyright © 2016 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures

References
-
- Swerdlow S.H., Campo E., Harris N.L., Jaffe E.S., Pileri S.A., Stein H. fourth edition. International Agency for Research on Cancer; Lyon, France: 2008. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues.
-
- Vardiman J.W., Thiele J., Arber D.A., Brunning R.D., Borowitz M.J., Porwit A. The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia: rationale and important changes. Blood. 2009;114(July (5)):937–951. - PubMed
-
- Jaffe E.S., Harris Nancy, Lee Stein, Harald Vardiman. IARC Press; Oxford University Press (distributor); Lyon, Oxford: 2001. James Pathology and Genetics of Tumours of Haematopoietic and Lymphoid Tissues.
-
- World Health Organization . World health organization; 2015. International Statistical Classification of Diseases and Related Health Problems ICD-10 Version:2015 [Internet]. ICD-10 Version:2015. ( http://apps.who.int/classifications/icd10/browse/2015/en: Available from: http://apps.who.int/classifications/icd10/browse/2015/en.)
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
