

Nonnucleoside Reverse-transcriptase Inhibitor- vs Ritonavir-boosted Protease Inhibitor-based Regimens for Initial Treatment of HIV Infection: A Systematic Review and Metaanalysis of Randomized Trials
- PMID: 27090986
- PMCID: PMC6276924
- DOI: 10.1093/cid/ciw236
Nonnucleoside Reverse-transcriptase Inhibitor- vs Ritonavir-boosted Protease Inhibitor-based Regimens for Initial Treatment of HIV Infection: A Systematic Review and Metaanalysis of Randomized Trials
Abstract
Background: Previous studies suggest that nonnucleoside reverse-transcriptase inhibitors (NNRTIs) cause faster virologic suppression, while ritonavir-boosted protease inhibitors (PI/r) recover more CD4 cells. However, individual trials have not been powered to compare clinical outcomes.
Methods: We searched databases to identify randomized trials that compared NNRTI- vs PI/r-based initial therapy. A metaanalysis calculated risk ratios (RRs) or mean differences (MDs), as appropriate. Primary outcome was death or progression to AIDS. Secondary outcomes were death, progression to AIDS, and treatment discontinuation. We calculated RR of virologic suppression and MD for an increase in CD4 cells at week 48.
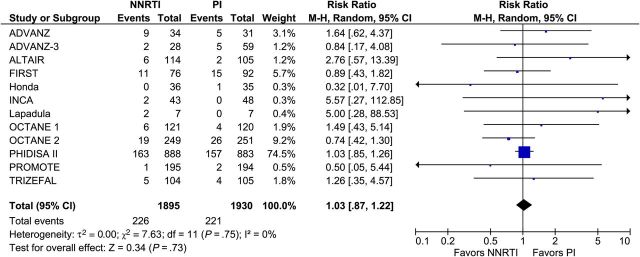
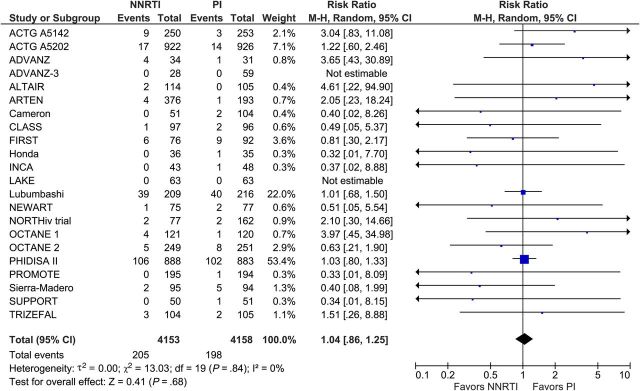
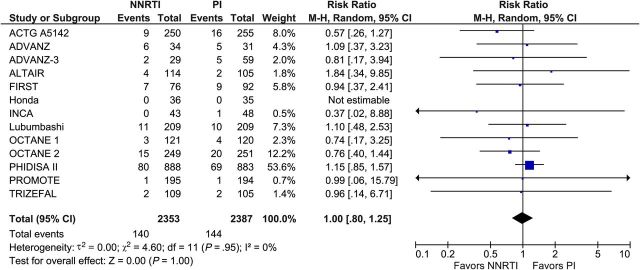
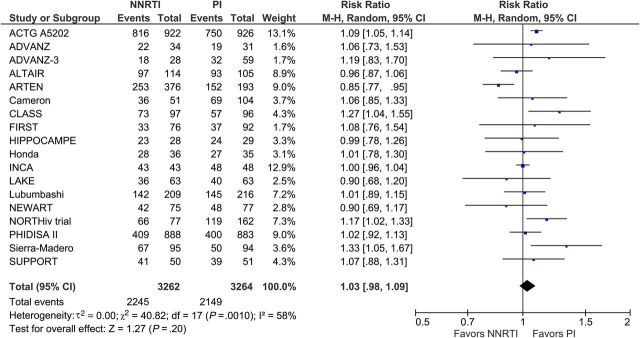
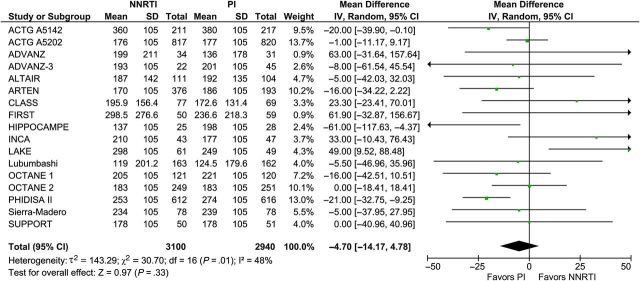
Results: We included 29 trials with 9047 participants. Death or progression to AIDS occurred in 226 participants in the NNRTI arm and in 221 in the PI/r arm (RR, 1.03; 95% confidence interval, .87-1.22; 12 trials; n = 3825), death in 205 participants in the NNRTI arm vs 198 in the PI/r arm (1.04; 0.86-1.25; 22 trials; n = 8311), and progression to AIDS in 140 participants in the NNRTI arm vs 144 in the PI/r arm (1.00; 0.80-1.25; 13 trials; n = 4740). Overall treatment discontinuation (1.12; 0.93-1.35; 24 trials; n = 8249) and from toxicity (1.21; 0.87-1.68; 21 trials; n = 6195) were comparable, but discontinuation due to virologic failure was more common with NNRTI (1.58; 0.91-2.74; 17 trials; n = 5371). At week 48, there was no difference between NNRTI and PI/r in virologic suppression (RR, 1.03; 0.98-1.09) or CD4(+) recovery (MD, -4.7 cells; -14.2 to 4.8).
Conclusions: We found no difference in clinical and viro-immunologic outcomes between NNRTI- and PI/r-based therapy.
Keywords: HIV; antiretroviral therapy; metaanalysis; nonnucleoside reverse transcriptase inhibitor; protease inhibitor.
© The Author 2016. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail journals.permissions@oup.com.
Figures
References
-
- Palella FJ Jr, Delaney KM, Moorman AC et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med 1998; 338:853–60. - PubMed
-
- Mocroft A, Vella S, Benfield TL et al. Changing patterns of mortality across Europe in patients infected with HIV-1. EuroSIDA Study Group. Lancet 1998; 352:1725–30. - PubMed
-
- Department of Health and Human Services Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Available at: http://aidsinfo.nih.gov/contentfiles/lvguidelines/AdultandAdolescentGL.pdf Accessed 30 November 2015.
-
- European AIDS Clinical Society 2015. European Guidelines for treatment of HIV-infected adults in Europe. Available at: http://www.eacsociety.org/files/2015_eacsguidelines_8.0-english_revised-... Accessed 30 November 2015.
-
- British HIV Association. British HIV Association guidelines for the treatment of HIV-1-positive adults with antiretroviral therapy 2015. Available at: http://www.bhiva.org/documents/Guidelines/Treatment/2015/2015-treatment-... Accessed 30 November 2015. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
