

Validated Risk Score for Predicting 6-Month Mortality in Infective Endocarditis
- PMID: 27091179
- PMCID: PMC4859286
- DOI: 10.1161/JAHA.115.003016
Validated Risk Score for Predicting 6-Month Mortality in Infective Endocarditis
Abstract
Background: Host factors and complications have been associated with higher mortality in infective endocarditis (IE). We sought to develop and validate a model of clinical characteristics to predict 6-month mortality in IE.
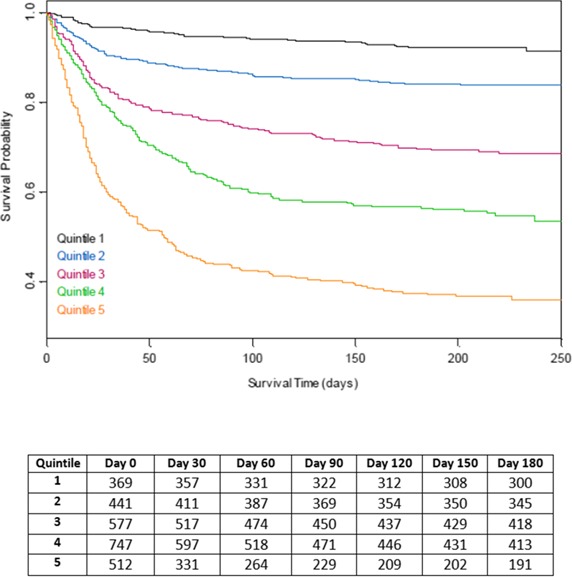
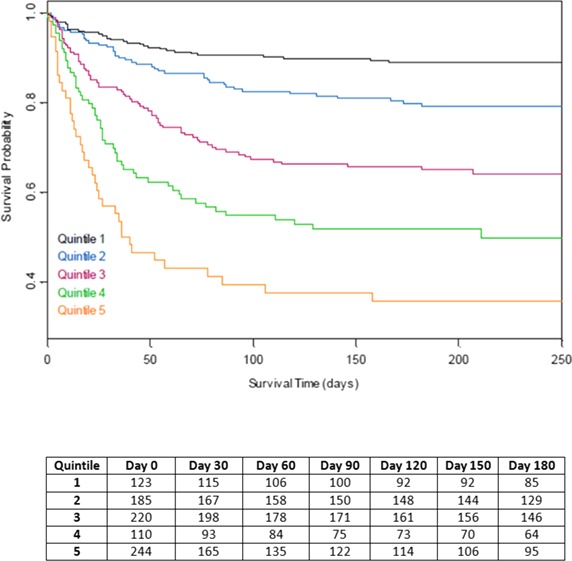
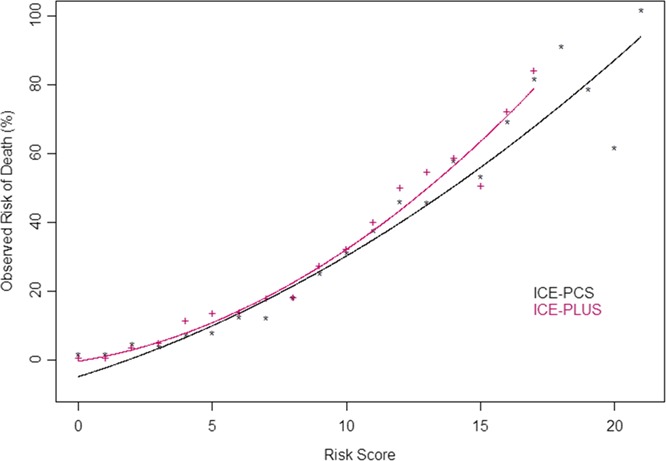
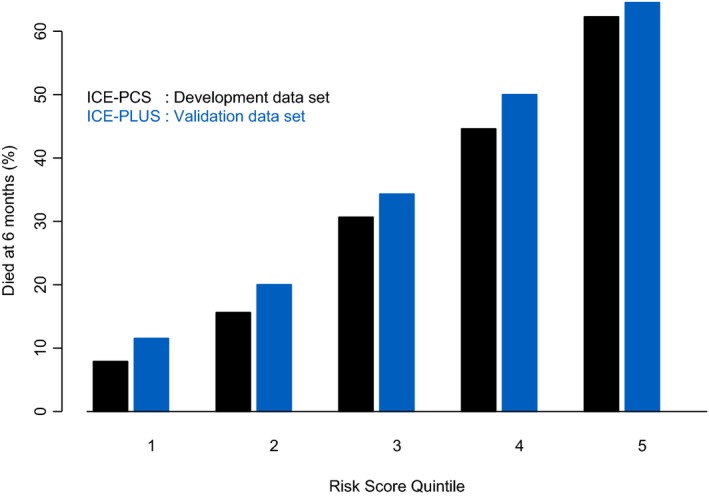
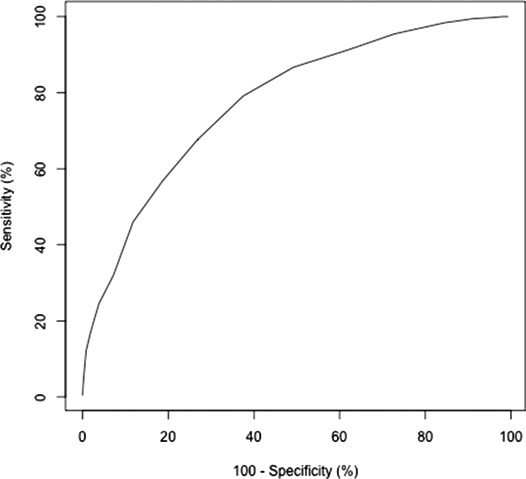
Methods and results: Using a large multinational prospective registry of definite IE (International Collaboration on Endocarditis [ICE]-Prospective Cohort Study [PCS], 2000-2006, n=4049), a model to predict 6-month survival was developed by Cox proportional hazards modeling with inverse probability weighting for surgery treatment and was internally validated by the bootstrapping method. This model was externally validated in an independent prospective registry (ICE-PLUS, 2008-2012, n=1197). The 6-month mortality was 971 of 4049 (24.0%) in the ICE-PCS cohort and 342 of 1197 (28.6%) in the ICE-PLUS cohort. Surgery during the index hospitalization was performed in 48.1% and 54.0% of the cohorts, respectively. In the derivation model, variables related to host factors (age, dialysis), IE characteristics (prosthetic or nosocomial IE, causative organism, left-sided valve vegetation), and IE complications (severe heart failure, stroke, paravalvular complication, and persistent bacteremia) were independently associated with 6-month mortality, and surgery was associated with a lower risk of mortality (Harrell's C statistic 0.715). In the validation model, these variables had similar hazard ratios (Harrell's C statistic 0.682), with a similar, independent benefit of surgery (hazard ratio 0.74, 95% CI 0.62-0.89). A simplified risk model was developed by weight adjustment of these variables.
Conclusions: Six-month mortality after IE is ≈25% and is predicted by host factors, IE characteristics, and IE complications. Surgery during the index hospitalization is associated with lower mortality but is performed less frequently in the highest risk patients. A simplified risk model may be used to identify specific risk subgroups in IE.
Keywords: infection; mortality; prognosis; surgery; valves.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Murdoch DR, Corey GR, Hoen B, Miro JM, Fowler VG Jr, Bayer AS, Karchmer AW, Olaison L, Pappas PA, Moreillon P, Chambers ST, Chu VH, Falco V, Holland DJ, Jones P, Klein JL, Raymond NJ, Read KM, Tripodi MF, Utili R, Wang A, Woods CW, Cabell CH. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the International Collaboration on Endocarditis‐Prospective Cohort Study. Arch Intern Med. 2009;169:463–473. - PMC - PubMed
-
- Benito N, Miro JM, de Lazzari E, Cabell CH, del Rio A, Altclas J, Commerford P, Delahaye F, Dragulescu S, Giamarellou H, Habib G, Kamarulzaman A, Kumar AS, Nacinovich FM, Suter F, Tribouilloy C, Venugopal K, Moreno A, Fowler VG Jr. Health care‐associated native valve endocarditis: importance of non‐nosocomial acquisition. Ann Intern Med. 2009;150:586–594. - PMC - PubMed
-
- Fowler VG Jr, Miro JM, Hoen B, Cabell CH, Abrutyn E, Rubinstein E, Corey GR, Spelman D, Bradley SF, Barsic B, Pappas PA, Anstrom KJ, Wray D, Fortes CQ, Anguera I, Athan E, Jones P, van der Meer JT, Elliott TS, Levine DP, Bayer AS. Staphylococcus aureus endocarditis: a consequence of medical progress. JAMA. 2005;293:3012–3021. - PubMed
-
- Thuny F, Giorgi R, Habachi R, Ansaldi S, Le Dolley Y, Casalta JP, Avierinos JF, Riberi A, Renard S, Collart F, Raoult D, Habib G. Excess mortality and morbidity in patients surviving infective endocarditis. Am Heart J. 2012;164:94–101. - PubMed
-
- Shih CJ, Chu H, Chao PW, Lee YJ, Kuo SC, Li SY, Tarng DC, Yang CY, Yang WC, Ou SM, Chen YT. Long‐term clinical outcome of major adverse cardiac events in survivors of infectious endocarditis: a nationwide population‐based study. Circulation. 2014;130:1684–1691. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
