

Endovascular treatment versus medical care alone for ischaemic stroke: systematic review and meta-analysis
- PMID: 27091337
- PMCID: PMC4834754
- DOI: 10.1136/bmj.i1754
Endovascular treatment versus medical care alone for ischaemic stroke: systematic review and meta-analysis
Abstract
Objectives: To evaluate the efficacy and safety of endovascular treatment, particularly adjunctive intra-arterial mechanical thrombectomy, in patients with ischaemic stroke.
Design: Systematic review and meta-analysis.
Data sources: Medline, Embase, Cochrane Central Register of Controlled Trials, Web of Science, SciELO, LILACS, and clinical trial registries from inception to December 2015. Reference lists were crosschecked.
Eligibility criteria for selecting studies: Randomised controlled trials in adults aged 18 or more with ischaemic stroke comparing endovascular treatment, including thrombectomy, with medical care alone, including intravenous recombinant tissue plasminogen activator (rt-PA). Trial endpoints were functional outcome (modified Rankin scale scores of ≤2) and mortality at 90 days after onset of symptoms. No language or time restrictions applied.
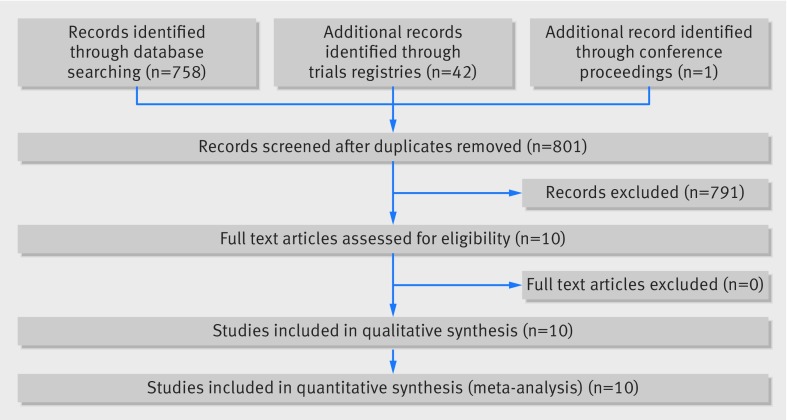
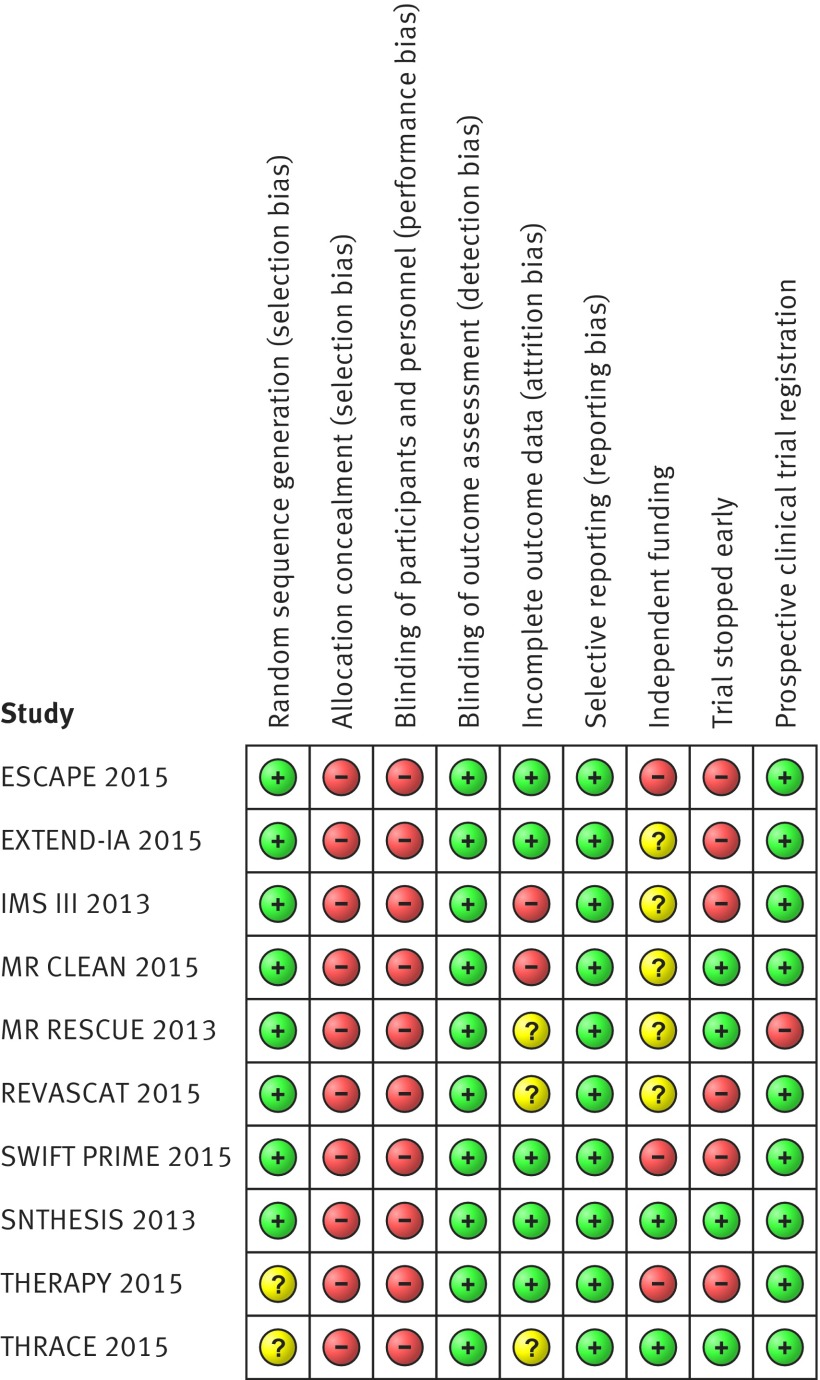
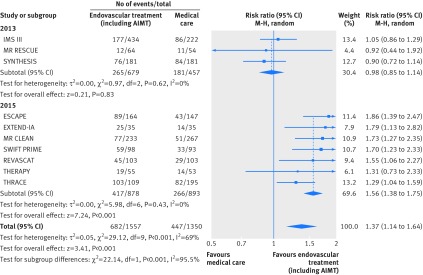
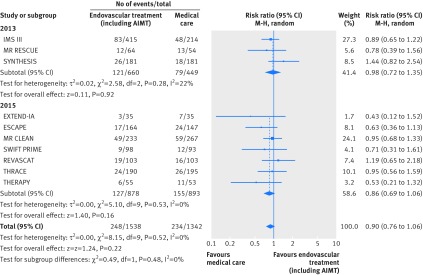
Results: 10 randomised controlled trials (n=2925) were included. In pooled analysis endovascular treatment, including thrombectomy, was associated with a higher proportion of patients experiencing good (modified Rankin scale scores ≤2) and excellent (scores ≤1) outcomes 90 days after stroke, without differences in mortality or rates for symptomatic intracranial haemorrhage, compared with patients randomised to medical care alone, including intravenous rt-PA. Heterogeneity was high among studies. The more recent studies (seven randomised controlled trials, published or presented in 2015) proved better suited to evaluate the effect of adjunctive intra-arterial mechanical thrombectomy on its index disease owing to more accurate patient selection, intravenous rt-PA being administered at a higher rate and earlier, and the use of more efficient thrombectomy devices. In most of these studies, more than 86% of the patients were treated with stent retrievers, and rates of recanalisation were higher (>58%) than previously reported. Subgroup analysis of these seven studies yielded a risk ratio of 1.56 (95% confidence interval 1.38 to 1.75) for good functional outcomes and 0.86 (0.69 to 1.06) for mortality, without heterogeneity among the results of the studies. All trials were open label. Risk of bias was moderate across studies. The full results of two trials are yet to be published.
Conclusions: Moderate to high quality evidence suggests that compared with medical care alone in a selected group of patients endovascular thrombectomy as add-on to intravenous thrombolysis performed within six to eight hours after large vessel ischaemic stroke in the anterior circulation provides beneficial functional outcomes, without increased detrimental effects.
Systematic review registration: PROSPERO CRD42015019340.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Endovascular treatment for stroke.BMJ. 2016 Apr 18;353:i2098. doi: 10.1136/bmj.i2098. BMJ. 2016. PMID: 27089891 No abstract available.
-
[Endovascular thrombectomy improves functional outcome of ischemic stroke patients].Dtsch Med Wochenschr. 2016 Jun;141(12):848. doi: 10.1055/s-0042-108536. Epub 2016 Jun 15. Dtsch Med Wochenschr. 2016. PMID: 27305296 German. No abstract available.
References
-
- Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380:2095-128. 10.1016/S0140-6736(12)61728-0 pmid:23245604. - DOI - PMC - PubMed
-
- Kissela BM, Khoury JC, Alwell K, et al. Age at stroke: temporal trends in stroke incidence in a large, biracial population. Neurology 2012;79:1781-7. 10.1212/WNL.0b013e318270401d pmid:23054237. - DOI - PMC - PubMed
-
- Thrift AG, Cadilhac DA, Thayabaranathan T, et al. Global stroke statistics. Int J Stroke 2014;9:6-18. 10.1111/ijs.12245 pmid:24350870. - DOI - PubMed
-
- Ueda T, Sakaki S, Kumon Y, Ohta S. Multivariable analysis of predictive factors related to outcome at 6 months after intra-arterial thrombolysis for acute ischemic stroke. Stroke 1999;30:2360-5. 10.1161/01.STR.30.11.2360 pmid:10548671. - DOI - PubMed
-
- Wardlaw JM, Murray V, Berge E, del Zoppo GJ. Thrombolysis for acute ischaemic stroke. Cochrane Database Syst Rev 2014;7:CD000213.pmid:25072528. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical