

Randomized phase 2 study: elotuzumab plus bortezomib/dexamethasone vs bortezomib/dexamethasone for relapsed/refractory MM
- PMID: 27091875
- PMCID: PMC4900953
- DOI: 10.1182/blood-2016-01-694604
Randomized phase 2 study: elotuzumab plus bortezomib/dexamethasone vs bortezomib/dexamethasone for relapsed/refractory MM
Abstract
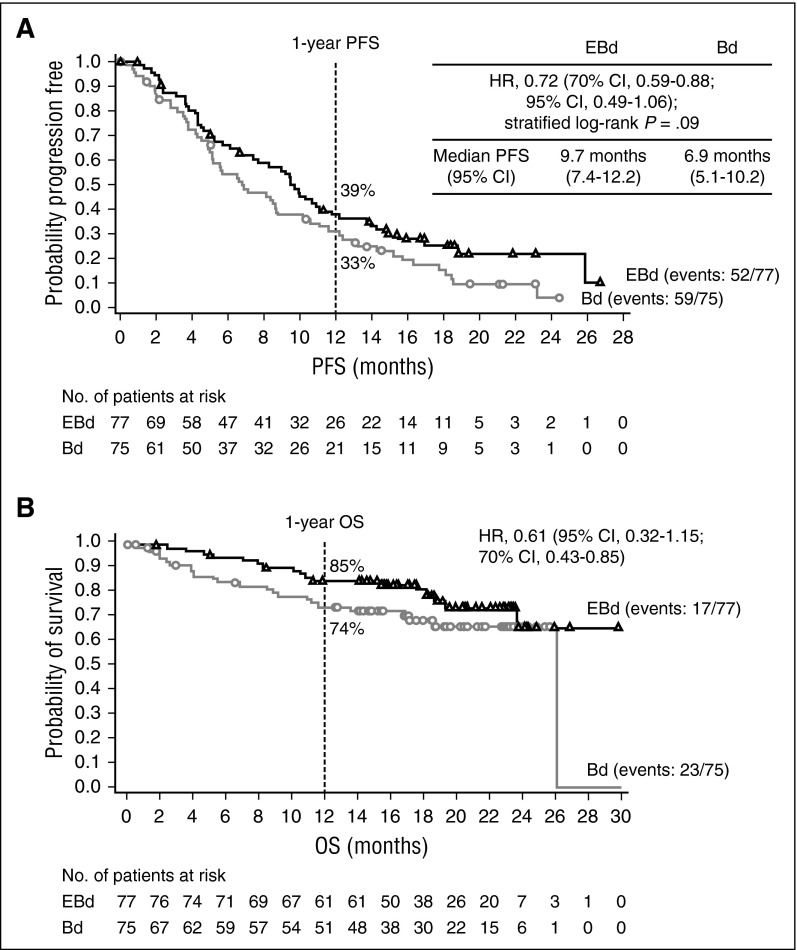
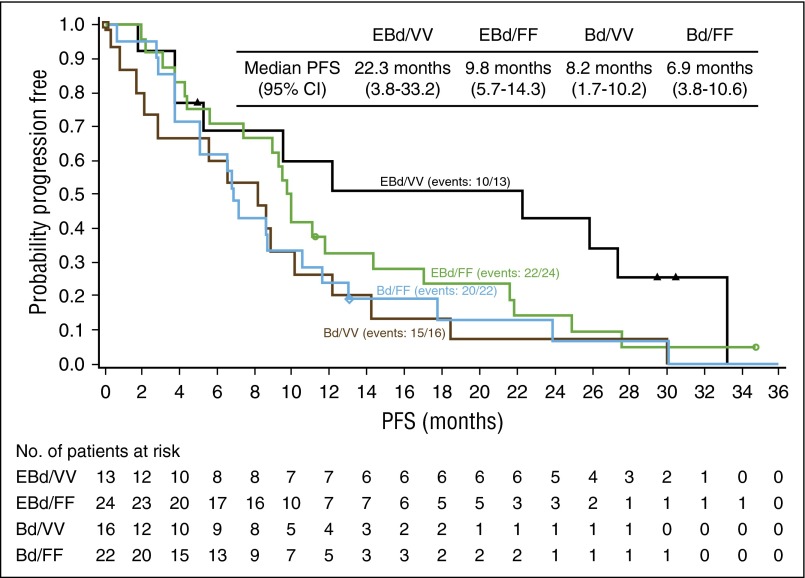
In this proof-of-concept, open-label, phase 2 study, patients with relapsed/refractory multiple myeloma (RRMM) received elotuzumab with bortezomib and dexamethasone (EBd) or bortezomib and dexamethasone (Bd) until disease progression/unacceptable toxicity. Primary endpoint was progression-free survival (PFS); secondary/exploratory endpoints included overall response rate (ORR) and overall survival (OS). Two-sided 0.30 significance level was specified (80% power, 103 events) to detect hazard ratio (HR) of 0.69. Efficacy and safety analyses were performed on all randomized patients and all treated patients, respectively. Of 152 randomized patients (77 EBd, 75 Bd), 150 were treated (75 EBd, 75 Bd). PFS was greater with EBd vs Bd (HR, 0.72; 70% confidence interval [CI], 0.59-0.88; stratified log-rank P = .09); median PFS was longer with EBd (9.7 months) vs Bd (6.9 months). In an updated analysis, EBd-treated patients homozygous for the high-affinity FcγRIIIa allele had median PFS of 22.3 months vs 9.8 months in EBd-treated patients homozygous for the low-affinity allele. ORR was 66% (EBd) vs 63% (Bd). Very good partial response or better occurred in 36% of patients (EBd) vs 27% (Bd). Early OS results, based on 40 deaths, revealed an HR of 0.61 (70% CI, 0.43-0.85). To date, 60 deaths have occurred (28 EBd, 32 Bd). No additional clinically significant adverse events occurred with EBd vs Bd. Grade 1/2 infusion reaction rate was low (5% EBd) and mitigated with premedication. In patients with RRMM, elotuzumab, an immunostimulatory antibody, appears to provide clinical benefit without added clinically significant toxicity when combined with Bd vs Bd alone. Registered to ClinicalTrials.gov as NCT01478048.
© 2016 by The American Society of Hematology.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015;65(1):5–29. - PubMed
-
- Smith BD, Smith GL, Hurria A, Hortobagyi GN, Buchholz TA. Future of cancer incidence in the United States: burdens upon an aging, changing nation. J Clin Oncol. 2009;27(17):2758–2765. - PubMed
-
- National Comprehensive Cancer Network (NCCN) NCCN Clinical Practice Guidelines for Treatment of Cancer by Site: Multiple Myeloma. Version 2.2016, September 22, 2015. http://www.nccn.org/professionals/physician_gls/f_guidelines.asp. Accessed December 15, 2015.
-
- Antonia SJ, Larkin J, Ascierto PA. Immuno-oncology combinations: a review of clinical experience and future prospects. Clin Cancer Res. 2014;20(24):6258–6268. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
