

How to Acquire Cardiac Volumes for Sonographic Examination of the Fetal Heart: Part 2
- PMID: 27091912
- PMCID: PMC8475629
- DOI: 10.7863/ultra.16.01082
How to Acquire Cardiac Volumes for Sonographic Examination of the Fetal Heart: Part 2
Abstract
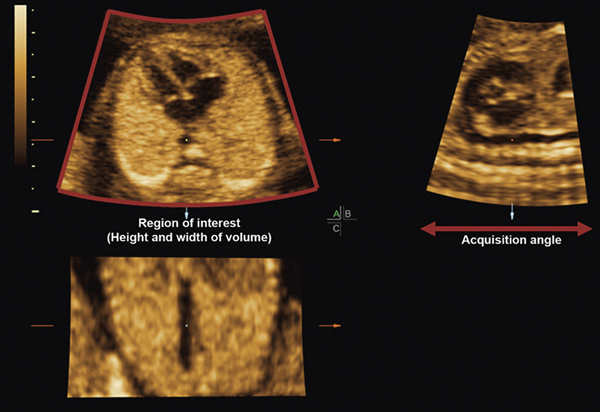
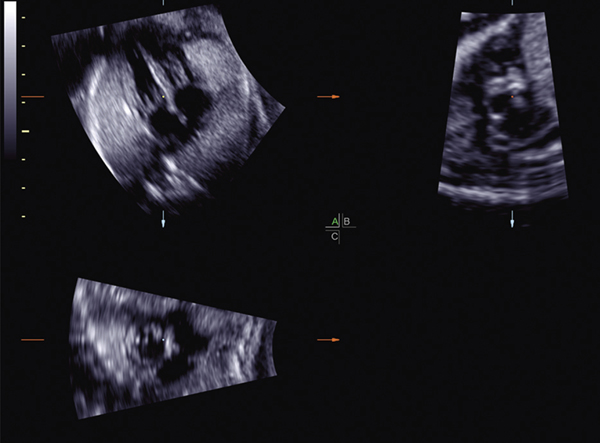
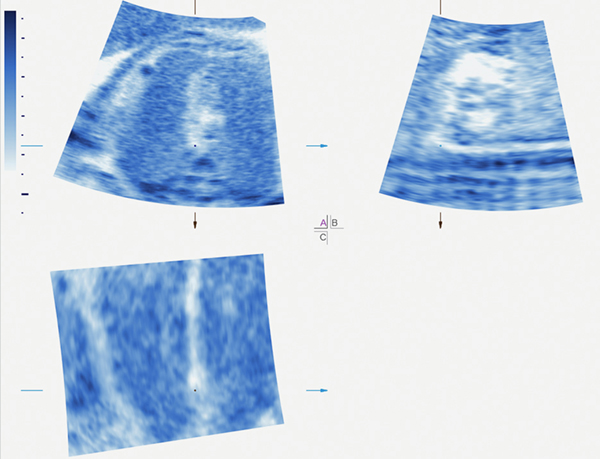
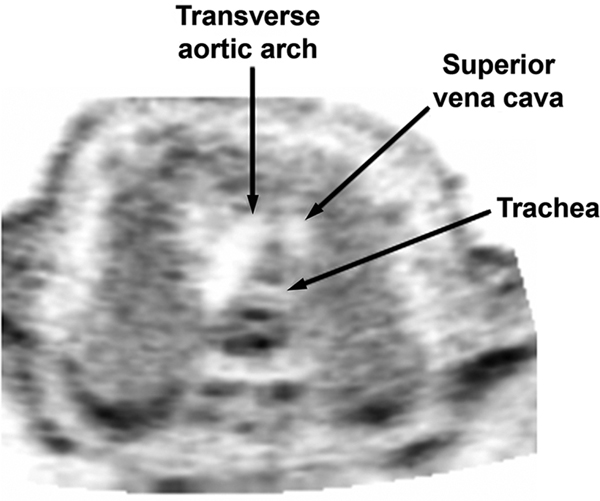
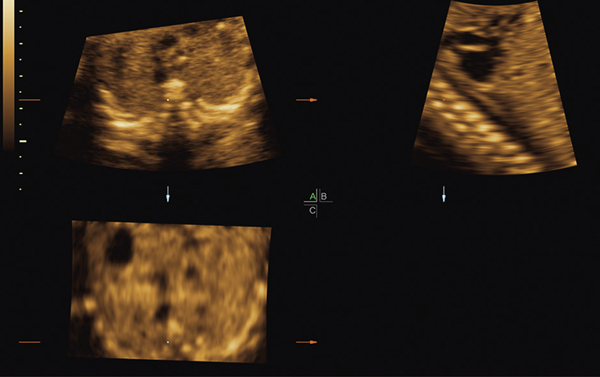
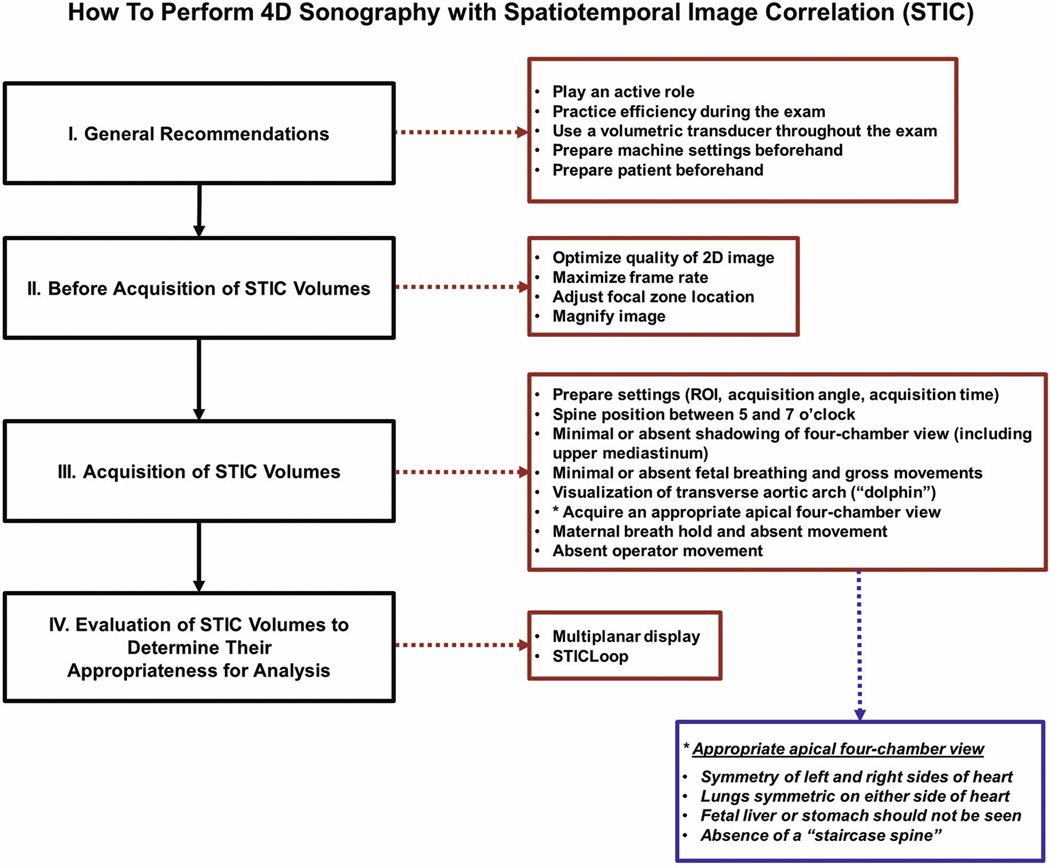
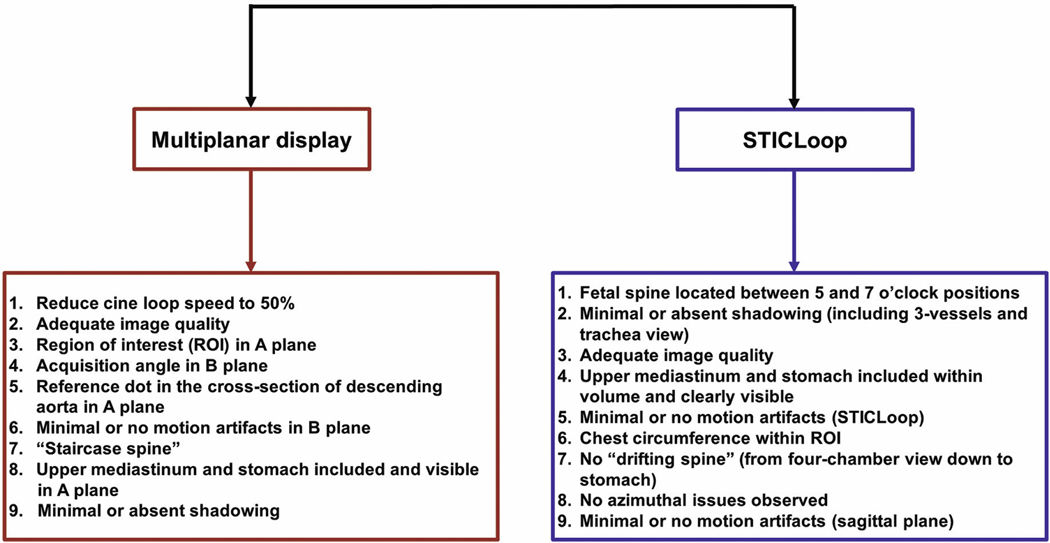
The effective performance of fetal cardiac examination using spatiotemporal image correlation (STIC) technology requires 2 essential steps: volume acquisition and postprocessing. An important prerequisite is training sonologists to acquire high-quality volume data sets so that when analyzed, such volumes are informative. This article is part 2 of a series on 4-dimensional sonography with STIC. Part 1 focused on STIC technology and its features, the importance of operator training/experience and acquisition of high-quality STIC volumes, factors that affect STIC volume acquisition rates, and general recommendations on performing 4D sonography with STIC. In part 2, we discuss a detailed and practical stepwise approach for STIC volume acquisition, along with methods to determine whether such volumes are appropriate for analysis.
Keywords: 4-dimensional; STICLoop; fetal echocardiography; fetus; spatiotemporal image correlation; ultrasound.
© 2016 by the American Institute of Ultrasound in Medicine.
Figures


Similar articles
-
How to Acquire Cardiac Volumes for Sonographic Examination of the Fetal Heart: Part 1.J Ultrasound Med. 2016 May;35(5):1021-42. doi: 10.7863/ultra.16.01081. Epub 2016 Apr 18. J Ultrasound Med. 2016. PMID: 27091914 Free PMC article.
-
Prospective evaluation of the fetal heart using Fetal Intelligent Navigation Echocardiography (FINE).Ultrasound Obstet Gynecol. 2016 Apr;47(4):450-9. doi: 10.1002/uog.15676. Epub 2016 Mar 10. Ultrasound Obstet Gynecol. 2016. PMID: 26278116 Free PMC article.
-
A systematic analysis of the feasibility of four-dimensional ultrasound imaging using spatiotemporal image correlation in routine fetal echocardiography.Ultrasound Obstet Gynecol. 2008 Jun;31(6):625-32. doi: 10.1002/uog.5351. Ultrasound Obstet Gynecol. 2008. PMID: 18504769
-
Fetal cardiac function by three-dimensional ultrasound using 4D-STIC and VOCAL - an update.J Ultrason. 2019 Dec;19(79):287-294. doi: 10.15557/JoU.2019.0043. Epub 2019 Dec 31. J Ultrason. 2019. PMID: 32021711 Free PMC article. Review.
-
A "holistic" sonographic view on congenital heart disease: How automatic reconstruction using fetal intelligent navigation echocardiography eases unveiling of abnormal cardiac anatomy part II-Left heart anomalies.Echocardiography. 2021 May;38(5):777-789. doi: 10.1111/echo.15037. Epub 2021 Mar 29. Echocardiography. 2021. PMID: 33778977 Review.
Cited by
-
How to Acquire Cardiac Volumes for Sonographic Examination of the Fetal Heart: Part 1.J Ultrasound Med. 2016 May;35(5):1021-42. doi: 10.7863/ultra.16.01081. Epub 2016 Apr 18. J Ultrasound Med. 2016. PMID: 27091914 Free PMC article.
-
Fetal intelligent navigation echocardiography (FINE) has superior performance compared to manual navigation of the fetal heart by non-expert sonologists.J Perinat Med. 2022 Dec 7;51(4):477-491. doi: 10.1515/jpm-2022-0387. Print 2023 May 25. J Perinat Med. 2022. PMID: 36474319 Free PMC article.
-
Optical ultrasound simulation-based training in obstetric sonography.J Matern Fetal Neonatal Med. 2022 Jul;35(13):2469-2484. doi: 10.1080/14767058.2020.1786519. Epub 2020 Jul 7. J Matern Fetal Neonatal Med. 2022. PMID: 32635783 Free PMC article. Review.
-
New and advanced features of fetal intelligent navigation echocardiography (FINE) or 5D heart.J Matern Fetal Neonatal Med. 2022 Apr;35(8):1498-1516. doi: 10.1080/14767058.2020.1759538. Epub 2020 May 6. J Matern Fetal Neonatal Med. 2022. PMID: 32375528 Free PMC article.
-
Prenatal Diagnosis of Dextrocardia with Complex Congenital Heart Disease Using Fetal Intelligent Navigation Echocardiography (FINE) and a Literature Review.Fetal Diagn Ther. 2018;43(4):304-316. doi: 10.1159/000468929. Epub 2017 Jun 23. Fetal Diagn Ther. 2018. PMID: 28641300 Free PMC article. Review.
References
-
- Viñals F, Poblete P, Giuliano A. Spatio-temporal image correlation (STIC): a new tool for the prenatal screening of congenital heart defects. Ultrasound Obstet Gynecol 2003; 22: 388–394. - PubMed
-
- DeVore GR, Falkensammer P, Sklansky MS, Platt LD. Spatiotemporal image correlation (STIC): new technology for evaluation of the fetal heart. Ultrasound Obstet Gynecol 2003; 22: 380–387. - PubMed
-
- Gonçalves LF, Lee W, Chaiworapongsa T, et al.Four-dimensional ultrasonography of the fetal heart with spatiotemporal image correlation. Am J Obstet Gynecol 2003; 189: 1792–1802. - PubMed
-
- Chaoui R, Hoffmann J, Heling KS. Three-dimensional (3D) and 4D color Doppler fetal echocardiography using spatio-temporal image correlation (STIC). Ultrasound Obstet Gynecol 2004; 23: 535–545. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
