

Clinically and pharmacologically relevant interactions of antidiabetic drugs
- PMID: 27092232
- PMCID: PMC4821002
- DOI: 10.1177/2042018816638050
Clinically and pharmacologically relevant interactions of antidiabetic drugs
Abstract
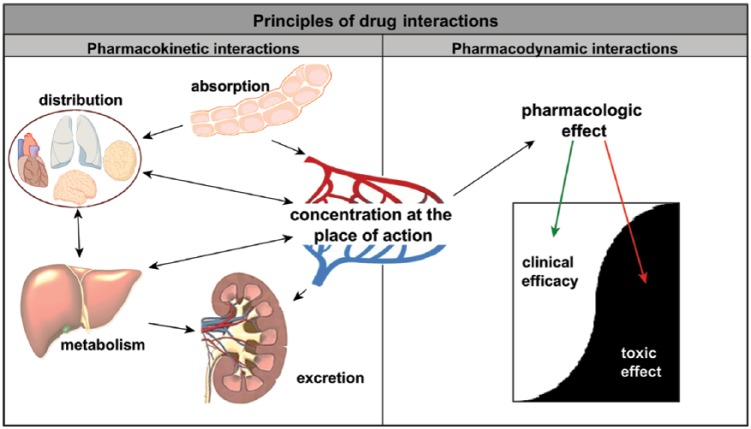
Patients with type 2 diabetes mellitus often require multifactorial pharmacological treatment due to different comorbidities. An increasing number of concomitantly taken medications elevate the risk of the patient experiencing adverse drug effects or drug interactions. Drug interactions can be divided into pharmacokinetic and pharmacodynamic interactions affecting cytochrome (CYP) enzymes, absorption properties, transporter activities and receptor affinities. Furthermore, nutrition, herbal supplements, patient's age and gender are of clinical importance. Relevant drug interactions are predominantly related to sulfonylureas, thiazolidinediones and glinides. Although metformin has a very low interaction potential, caution is advised when drugs that impair renal function are used concomitantly. With the exception of saxagliptin, dipeptidyl peptidase-4 (DPP-4) inhibitors also show a low interaction potential, but all drugs affecting the drug transporter P-glycoprotein should be used with caution. Incretin mimetics and sodium-glucose cotransporter-2 (SGLT-2) inhibitors comprise a very low interaction potential and are therefore recommended as an ideal combination partner from the clinical-pharmacologic point of view.
Keywords: adverse effects; diabetes mellitus; drug interactions; drug therapy; hypoglycemic agents; pharmacodynamic interactions; pharmacokinetic interactions.
Conflict of interest statement
Figures
References
-
- Amin M., Suksomboon N. (2014) Pharmacotherapy of type 2 diabetes mellitus: an update on drug-drug interactions. Drug Saf 37: 903–919. - PubMed
-
- Amori R., Lau J., Pittas A. (2007) Efficacy and safety of incretin therapy in type 2 diabetes: systematic review and meta-analysis. JAMA 298: 194–206. - PubMed
-
- Anderson R., Freedland K., Clouse R., Lustman P. (2001) The prevalence of comorbid depression in adults with diabetes: a meta-analysis. Diabetes Care 24: 1069–1078. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
