

Personal protective equipment for preventing highly infectious diseases due to exposure to contaminated body fluids in healthcare staff
- PMID: 27093058
- PMCID: PMC10068873
- DOI: 10.1002/14651858.CD011621.pub2
Personal protective equipment for preventing highly infectious diseases due to exposure to contaminated body fluids in healthcare staff
Update in
-
Personal protective equipment for preventing highly infectious diseases due to exposure to contaminated body fluids in healthcare staff.Cochrane Database Syst Rev. 2019 Jul 1;7(7):CD011621. doi: 10.1002/14651858.CD011621.pub3. Cochrane Database Syst Rev. 2019. Update in: Cochrane Database Syst Rev. 2020 Apr 15;4:CD011621. doi: 10.1002/14651858.CD011621.pub4. PMID: 31259389 Free PMC article. Updated.
Abstract
Background: In epidemics of highly infectious diseases, such as Ebola Virus Disease (EVD) or SARS, healthcare workers (HCW) are at much greater risk of infection than the general population, due to their contact with patients' contaminated body fluids. Contact precautions by means of personal protective equipment (PPE) can reduce the risk. It is unclear which type of PPE protects best, what is the best way to remove PPE, and how to make sure HCWs use PPE as instructed.
Objectives: To evaluate which type or component of full-body PPE and which method of donning or removing (doffing) PPE have the least risk of self-contamination or infection for HCWs, and which training methods most increase compliance with PPE protocols.
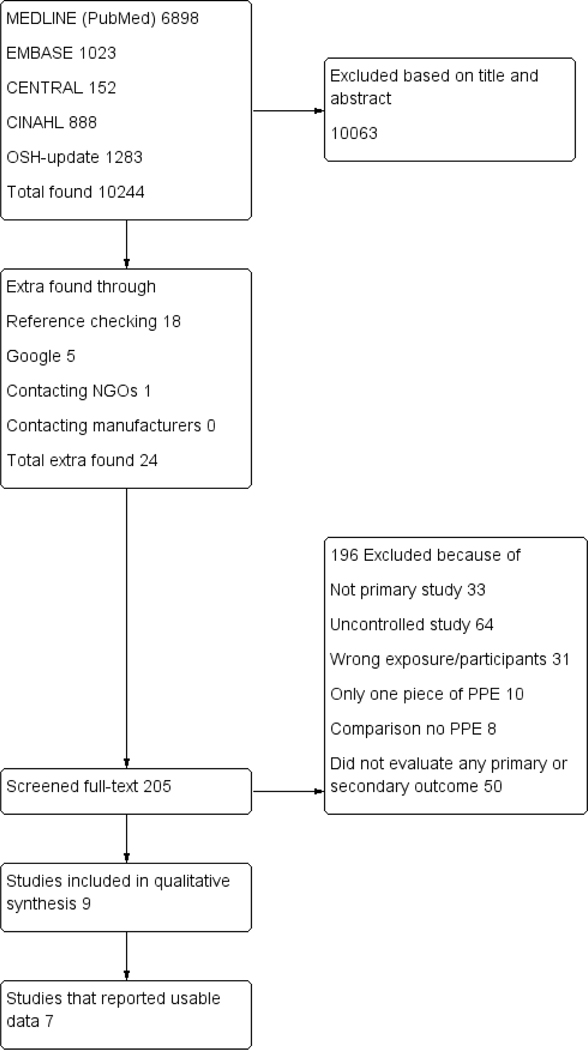
Search methods: We searched MEDLINE (PubMed up to 8 January 2016), Cochrane Central Register of Trials (CENTRAL up to 20 January 2016), EMBASE (embase.com up to 8 January 2016), CINAHL (EBSCOhost up to 20 January 2016), and OSH-Update up to 8 January 2016. We also screened reference lists of included trials and relevant reviews, and contacted NGOs and manufacturers of PPE.
Selection criteria: We included all eligible controlled studies that compared the effect of types or components of PPE in HCWs exposed to highly infectious diseases with serious consequences, such as EVD and SARS, on the risk of infection, contamination, or noncompliance with protocols. This included studies that simulated contamination with fluorescent markers or a non-pathogenic virus.We also included studies that compared the effect of various ways of donning or removing PPE, and the effects of various types of training in PPE use on the same outcomes.
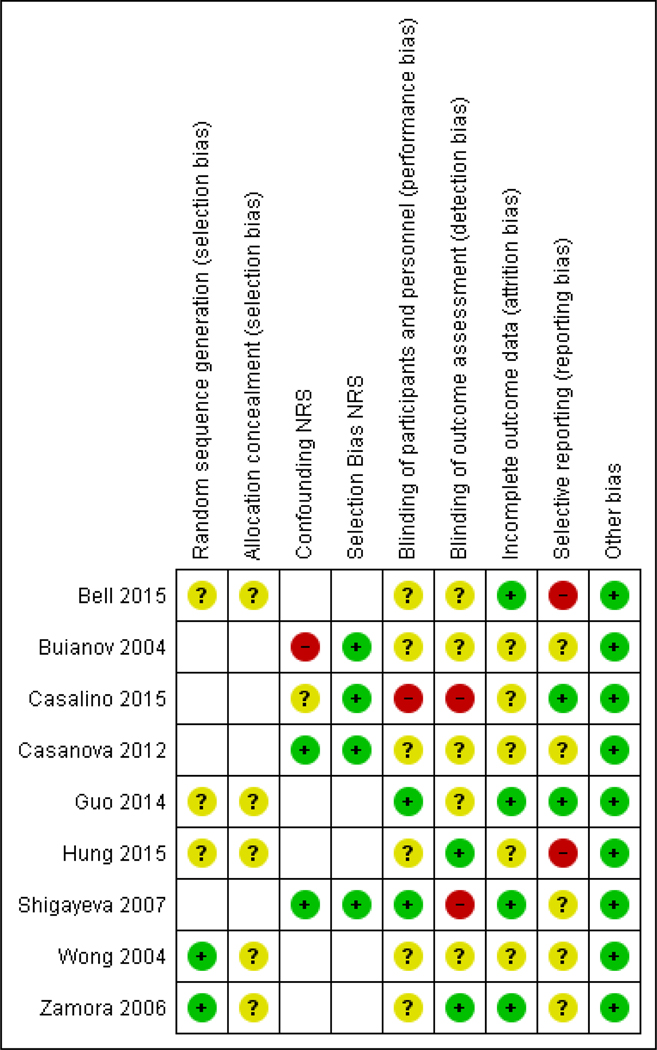
Data collection and analysis: Two authors independently selected studies, extracted data and assessed risk of bias in included trials. We intended to perform meta-analyses but we did not find sufficiently similar studies to combine their results.
Main results: We included nine studies with 1200 participants evaluating ten interventions. Of these, eight trials simulated the exposure with a fluorescent marker or virus or bacteria containing fluids. Five studies evaluated different types of PPE against each other but two did not report sufficient data. Another two studies compared different types of donning and doffing and three studies evaluated the effect of different types of training.None of the included studies reported a standardised classification of the protective properties against viral penetration of the PPE, and only one reported the brand of PPE used. None of the studies were conducted with HCWs exposed to EVD but in one study participants were exposed to SARS. Different types of PPE versus each otherIn simulation studies, contamination rates varied from 25% to 100% of participants for all types of PPE. In one study, PPE made of more breathable material did not lead to a statistically significantly different number of spots with contamination but did have greater user satisfaction (Mean Difference (MD) -0.46 (95% Confidence Interval (CI) -0.84 to -0.08, range 1 to 5, very low quality evidence). In another study, gowns protected better than aprons. In yet another study, the use of a powered air-purifying respirator protected better than a now outdated form of PPE. There were no studies on goggles versus face shields, on long- versus short-sleeved gloves, or on the use of taping PPE parts together. Different methods of donning and doffing procedures versus each otherTwo cross-over simulation studies (one RCT, one CCT) compared different methods for donning and doffing against each other. Double gloving led to less contamination compared to single gloving (Relative Risk (RR) 0.36; 95% CI 0.16 to 0.78, very low quality evidence) in one simulation study, but not to more noncompliance with guidance (RR 1.08; 95% CI 0.70 to 1.67, very low quality evidence). Following CDC recommendations for doffing led to less contamination in another study (very low quality evidence). There were no studies on the use of disinfectants while doffing. Different types of training versus each otherIn one study, the use of additional computer simulation led to less errors in doffing (MD -1.2, 95% CI -1.6 to -0.7) and in another study additional spoken instruction led to less errors (MD -0.9, 95% CI -1.4 to -0.4). One retrospective cohort study assessed the effect of active training - defined as face-to-face instruction - versus passive training - defined as folders or videos - on noncompliance with PPE use and on noncompliance with doffing guidance. Active training did not considerably reduce noncompliance in PPE use (Odds Ratio (OR) 0.63; 95% CI 0.31 to 1.30) but reduced noncompliance with doffing procedures (OR 0.45; 95% CI 0.21 to 0.98, very low quality evidence). There were no studies on how to retain the results of training in the long term or on resource use.The quality of the evidence was very low for all comparisons because of high risk of bias in studies, indirectness of evidence, and small numbers of participants. This means that it is likely that the true effect can be substantially different from the one reported here.
Authors' conclusions: We found very low quality evidence that more breathable types of PPE may not lead to more contamination, but may have greater user satisfaction. We also found very low quality evidence that double gloving and CDC doffing guidance appear to decrease the risk of contamination and that more active training in PPE use may reduce PPE and doffing errors more than passive training. However, the data all come from single studies with high risk of bias and we are uncertain about the estimates of effects.We need simulation studies conducted with several dozens of participants, preferably using a non-pathogenic virus, to find out which type and combination of PPE protects best, and what is the best way to remove PPE. We also need randomised controlled studies of the effects of one type of training versus another to find out which training works best in the long term. HCWs exposed to highly infectious diseases should have their use of PPE registered and should be prospectively followed for their risk of infection.
Conflict of interest statement
DECLARATIONS OF INTEREST
Jos Verbeek: None known.
Sharea Ijaz: None known.
Christina Mischke: None known.
Jani Ruotsalainen: None known.
F Selcen Kilinc Balci: None known.
Erja Mäkelä: None known.
Kaisa Neuvonen: None known.
Michael Edmond: I have given several lectures to non-profit professional associations (e.g. APIC) on topics related to infection control that in some instances provide an honorarium. None of these lectures were for industry.
Riitta Sauni: None known.
Raluca C Mihalache: None known.
Figures

References
References to studies included in this review
-
- Buianov VV, Kolesnikov NV, Malyshev NA, Suprun IP. [Use of new individual protection substances in Mel’tser boxes]. Vestnik Rossiĭskoĭ Akademii Meditsinskikh Nauk 2004;1:30–5. - PubMed
-
- Casalino E, Astocondor E, Sanchez JC, Diaz-Santana DE, Del Aquila C, Carrillo JP. Personal protective equipment for the Ebola virus disease: A comparison of 2 training programs. American Journal of Infection Control 2015;43(12):1281–7. - PubMed
References to studies excluded from this review
-
- Beam EL, Gibbs SG, Hewlett AL, Iwen PC, Nuss SL, Smith PW. Method for investigating nursing behaviors related to isolation care. American Journal of Infection Control 2014;42(11):1152–6. - PubMed
-
- Bearman GM, Marra AR, Sessler CN, Smith WR, Rosato A, Laplante JK, et al. A controlled trial of universal gloving versus contact precautions for preventing the transmission of multidrug-resistant organisms. American Journal of Infection Control 2007;35(10):650–5. - PubMed
-
- Belkin NL. The protectiveness of protective clothing. Infection Control and Hospital Epidemiology 1991;12(8):464–468. - PubMed
Additional references
-
- ANSI/AAMI. PB70: Liquid barrier performance and classification of protective apparel and drapes in health care facilities. Association for the Advancement of Medical Instrumentation; 2012.
-
- Australian National Health and Medical Research Council. Australian guidelines for the prevention and control of infection in healthcare. http://www.nhmrc.gov.au/book/html-australian-guidelines-prevention-and-c...2010. (accessed 8 December 2014).
-
- Campbell MK, Mollison J, Grimshaw JM. Cluster trials in implementation research: estimation of intracluster correlation coefficients and sample size. Statistics in Medicine 2001;20(3):391–9. - PubMed
-
- Centers for Disease Control and Prevention (CDC). Outbreak of severe acute respiratory syndrome - worldwide, 2003. Morbidity and Mortality Weekly Report 2003;52(11):226–8. - PubMed
-
- Center for Disease Control. Guidance on personal protective equipment to be used by healthcare workers during management of patients with Ebola virus disease in U.S. Hospitals, including procedures for putting on (donning) and removing (doffing). http://www.cdc.gov/vhf/ebola/hcp/procedures-for-ppe.html (accessed 8 December 2014).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous