

Loss of health related quality of life following low-trauma fractures in the elderly
- PMID: 27093957
- PMCID: PMC4837505
- DOI: 10.1186/s12877-016-0259-5
Loss of health related quality of life following low-trauma fractures in the elderly
Abstract
Background: To estimate the long-term change in health related quality of life (HRQoL) following low-trauma fractures among individuals receiving home care (HC) services or living in long-term care (LTC) facilities using linked healthcare administrative data from Ontario, Canada.
Methods: HRQoL was estimated using the Health Utility Index (HUI-2) with the InterRai Minimum Data Set (MDS), a mandatory questionnaire for LTC and HC in the province of Ontario (population 14 million). The HUI-2, a validated HRQoL instrument, allows the calculation of health utility where 0 represents death and 1 the best imaginable health state. For reference, the HUI-2 utility value for Canadians aged 80-84 years is 0.61 and the minimal clinically important difference is 0.03. The MDS was linked to Ontario acute care databases for fiscal years 2007-2011 to identify low-trauma fractures using ICD-10-CA codes. Regression models were used to identify predictors of change in HRQoL from pre-fracture levels to 3 years post fracture for several populations. Low-trauma fractures included hip, humerus, vertebral, wrist, multiple and other.
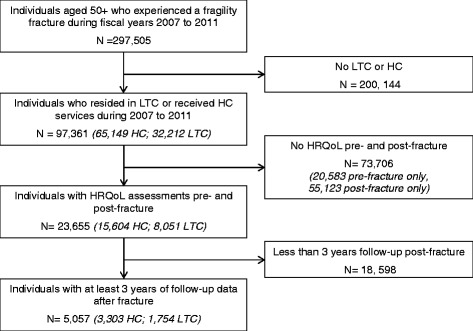
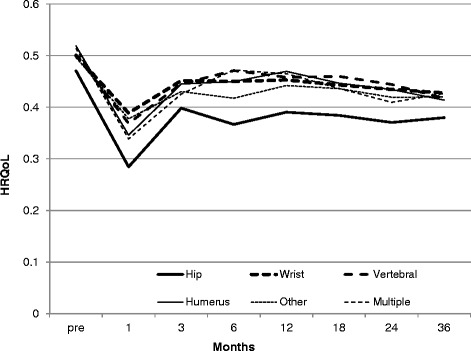
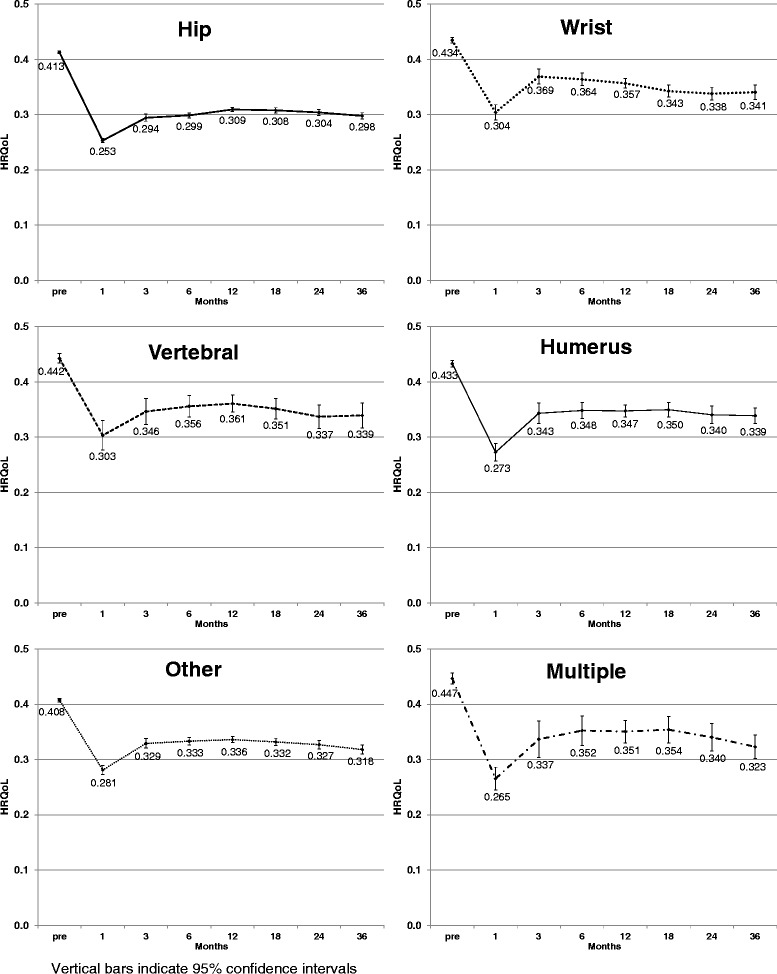
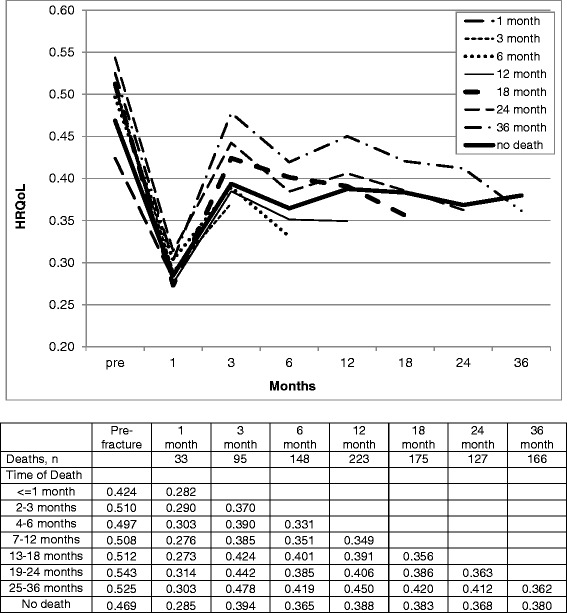
Results: Twenty-three thousand six-hundred fifty-five unique patients with low-trauma fractures were identified with pre- and post-fracture HRQoL assessments, of which 5057 individuals had at least 3 years of follow-up. Compared to patients receiving HC services (N = 3303), individuals residing in LTC (N = 1754) were older, taking more medications, and had more comorbidities. LTC patients had more hip fractures (49 % of total versus 29 %). For all fracture types, HRQoL decreased immediately following fracture. Although levels rebounded after the first month, HRQoL up to 36 months never returned to pre-fracture levels even for non-hip fracture. For both HC and LTC cohorts, clinically important and statistically significant decreases in HUI-2 utility scores were observed 36 months post fracture. Of the 6 HUI-2 domains, mobility had the largest impact on change in HRQoL. Regression analysis indicated that living with a musculoskeletal disorder or a neurological condition and living in LTC were associated with greater decrements in utility following a fracture.
Conclusions: Based on the analysis of one of the largest studies on HRQoL to date, among individuals living in LTC facilities or receiving HC services, fractures have a significant permanent impact on HRQoL up to 3 years following fracture.
Keywords: Fractures; Frail elderly; Health-related quality of life.
Figures
Similar articles
-
Comparative trends in incident fracture rates for all long-term care and community-dwelling seniors in Ontario, Canada, 2002-2012.Osteoporos Int. 2016 Mar;27(3):887-897. doi: 10.1007/s00198-015-3477-3. Epub 2016 Jan 22. Osteoporos Int. 2016. PMID: 26801930 Free PMC article.
-
Validation of a one year fracture prediction tool for absolute hip fracture risk in long term care residents.BMC Geriatr. 2018 Dec 27;18(1):320. doi: 10.1186/s12877-018-1010-1. BMC Geriatr. 2018. PMID: 30587140 Free PMC article.
-
Hip fracture rate and osteoporosis treatment in Ontario: A population-based retrospective cohort study.Arch Osteoporos. 2024 Jun 25;19(1):53. doi: 10.1007/s11657-024-01402-6. Arch Osteoporos. 2024. PMID: 38918265 Free PMC article.
-
Internal fixation implants for intracapsular hip fractures in older adults.Cochrane Database Syst Rev. 2021 Mar 9;3(3):CD013409. doi: 10.1002/14651858.CD013409.pub2. Cochrane Database Syst Rev. 2021. PMID: 33687067 Free PMC article.
-
Screening for the primary prevention of fragility fractures among adults aged 40 years and older in primary care: systematic reviews of the effects and acceptability of screening and treatment, and the accuracy of risk prediction tools.Syst Rev. 2023 Mar 21;12(1):51. doi: 10.1186/s13643-023-02181-w. Syst Rev. 2023. PMID: 36945065 Free PMC article.
Cited by
-
Quality of Life and Functional Independence of Hip Fracture Patients: Data from a Single Center Follow-Up Study in Sri Lanka.Ann Geriatr Med Res. 2021 Jun;25(2):98-104. doi: 10.4235/agmr.21.0016. Epub 2021 Jun 25. Ann Geriatr Med Res. 2021. PMID: 34120437 Free PMC article.
-
Benefits of a digital health technology for older nursing home residents. A de-novo cost-effectiveness model for digital health technologies to aid in the assessment of toileting and containment care needs.PLoS One. 2024 Jan 2;19(1):e0295846. doi: 10.1371/journal.pone.0295846. eCollection 2024. PLoS One. 2024. PMID: 38166006 Free PMC article.
-
Prognostic performance of clinical assessment tools following hip fracture in patients with chronic kidney disease.Int Urol Nephrol. 2021 Nov;53(11):2359-2367. doi: 10.1007/s11255-021-02798-7. Epub 2021 Mar 8. Int Urol Nephrol. 2021. PMID: 33686533 Free PMC article.
-
Health-related quality of life in men with osteoporosis: a systematic review and meta-analysis.Endocrine. 2021 Nov;74(2):270-280. doi: 10.1007/s12020-021-02792-0. Epub 2021 Jun 24. Endocrine. 2021. PMID: 34165773
-
Multi-detector computed tomography (MDCT) imaging: association of bone texture parameters with finite element analysis (FEA)-based failure load of single vertebrae and functional spinal units.Quant Imaging Med Surg. 2021 Jul;11(7):2955-2967. doi: 10.21037/qims-20-1156. Quant Imaging Med Surg. 2021. PMID: 34249626 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
