

Patterns of cortical thinning in nondemented Parkinson's disease patients
- PMID: 27094093
- PMCID: PMC5061099
- DOI: 10.1002/mds.26590
Patterns of cortical thinning in nondemented Parkinson's disease patients
Abstract
Background: Clinical variability in the Parkinson's disease phenotype suggests the existence of disease subtypes. We investigated whether distinct anatomical patterns of atrophy can be identified in Parkinson's disease using a hypothesis-free, data-driven approach based on cortical thickness data.
Methods: T1-weighted 3-tesla MRI and a comprehensive neuropsychological assessment were performed in a sample of 88 nondemented Parkinson's disease patients and 31 healthy controls. We performed a hierarchical cluster analysis of imaging data using Ward's linkage method. A general linear model with cortical thickness data was used to compare clustering groups.
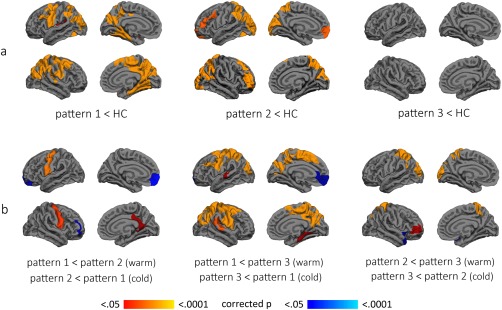
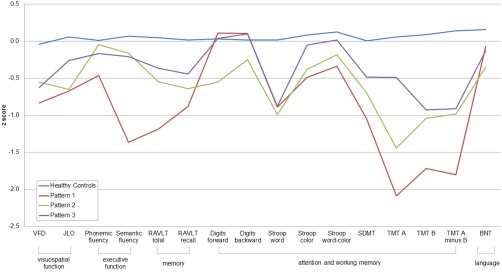
Results: We observed 3 patterns of cortical thinning in patients when compared with healthy controls. Pattern 1 (n = 30, 34.09%) consisted of cortical atrophy in bilateral precentral gyrus, inferior and superior parietal lobules, cuneus, posterior cingulate, and parahippocampal gyrus. These patients showed worse cognitive performance when compared with controls and the other 2 patterns. Pattern 2 (n = 29, 32.95%) consisted of cortical atrophy involving occipital and frontal as well as superior parietal areas and included patients with younger age at onset. Finally, in pattern 3 (n = 29, 32.95%), there was no detectable cortical thinning. Patients in the 3 patterns did not differ in disease duration, motor severity, dopaminergic medication doses, or presence of mild cognitive impairment.
Conclusions: Three cortical atrophy subtypes were identified in nondemented Parkinson's disease patients: (1) parieto-temporal pattern of atrophy with worse cognitive performance, (2) occipital and frontal cortical atrophy and younger disease onset, and (3) patients without detectable cortical atrophy. These findings may help identify prognosis markers in Parkinson's disease. © 2016 The Authors. Movement Disorders published by Wiley Periodicals, Inc. on behalf of International Parkinson and Movement Disorder Society.
Keywords: Parkinson disease; cluster analysis; cortical atrophy; magnetic resonance imaging; neuropsychology.
© 2016 The Authors. Movement Disorders published by Wiley Periodicals, Inc. on behalf of International Parkinson and Movement Disorder Society.
Figures

References
-
- Svenningsson P, Westman E, Ballard C, Aarsland D. Cognitive impairment in patients with Parkinson's disease: diagnosis, biomarkers, and treatment. Lancet Neurol 2012;11:697–707. - PubMed
-
- Van Rooden SM, Colas F, Martinez‐Martin P, et al. Clinical subtypes of Parkinson's disease. Mov Disord 2011;26(1):51–58. - PubMed
-
- Fereshtehnejad SM, Romenets SR, Anang JBM, Latreille V, Gagnon JF, Postuma RB. New clinical subtypes of parkinson disease and their longitudinal progression: a prospective cohort comparison with other phenotypes. JAMA Neurol 2015;72(8):1–11. - PubMed
-
- Dujardin K, Leentjens AFG, Langlois C, et al. The spectrum of cognitive disorders in Parkinson's disease: a data‐driven approach. Mov Disord 2013;28(2):183–189. - PubMed
-
- Daniel SE, Lees AJ. Parkinson's Disease Society Brain Bank, London: overview and research. J Neural Transm Suppl 1993;39:165–172. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
