

Disease-specific dynamic biomarkers selected by integrating inflammatory mediators with clinical informatics in ARDS patients with severe pneumonia
- PMID: 27095254
- PMCID: PMC4882347
- DOI: 10.1007/s10565-016-9322-4
Disease-specific dynamic biomarkers selected by integrating inflammatory mediators with clinical informatics in ARDS patients with severe pneumonia
Abstract
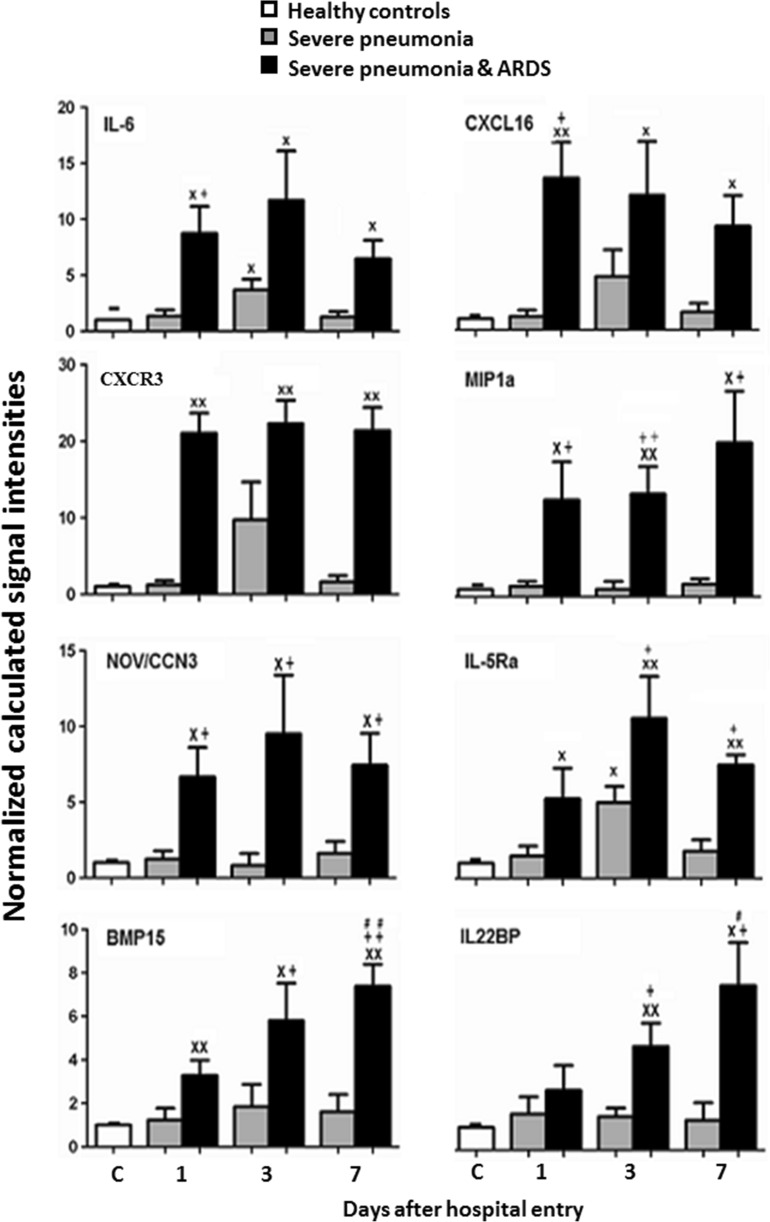
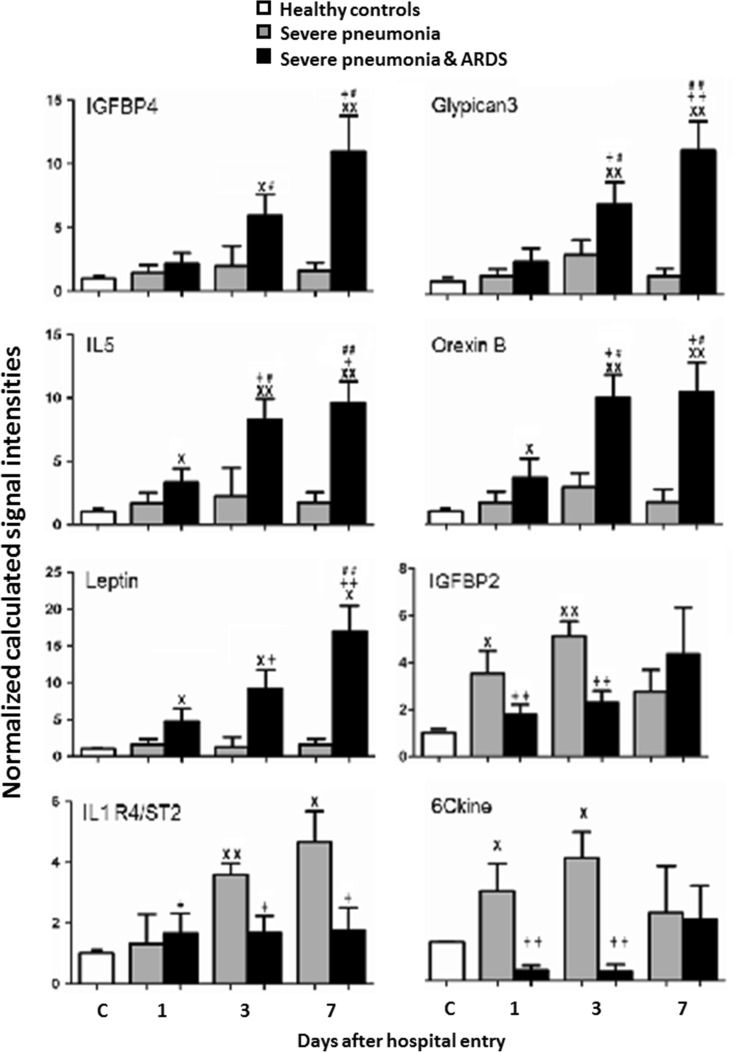
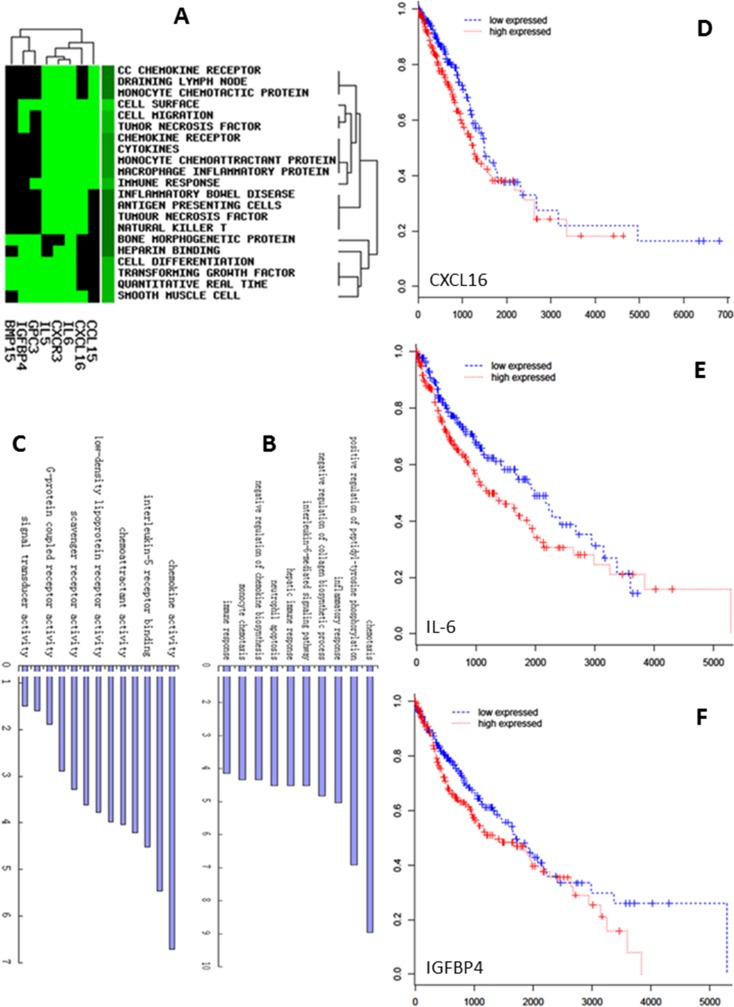
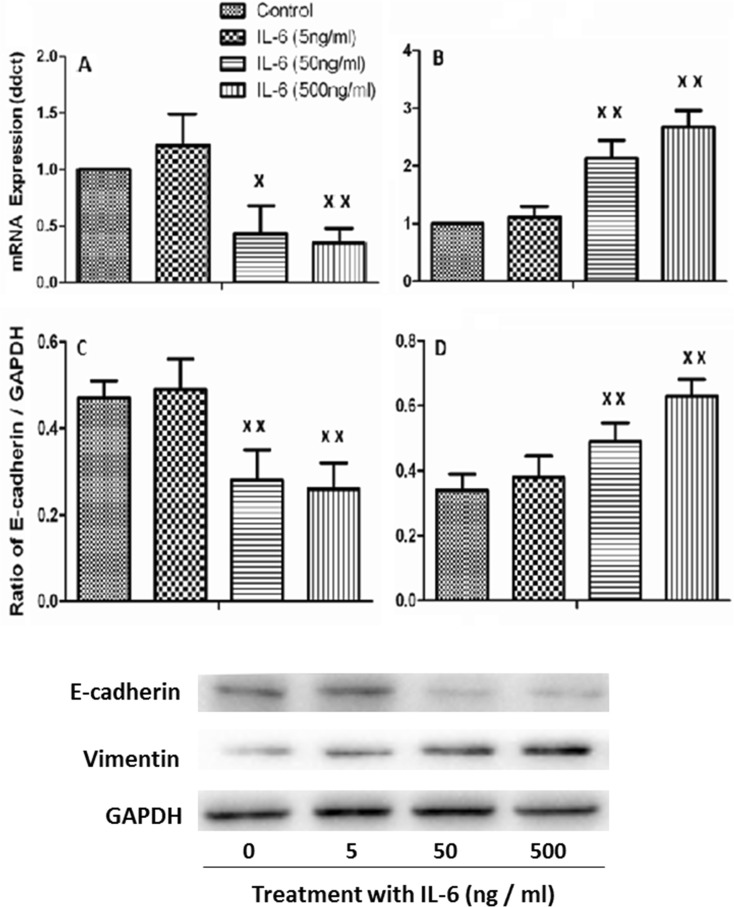
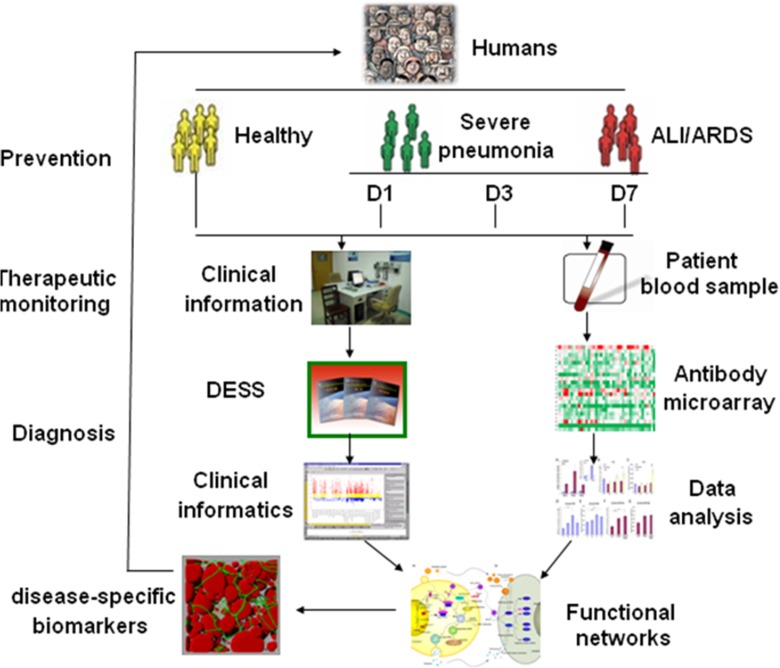
Acute respiratory distress syndrome (ARDS) is a heterogeneous syndrome that occurs as a result of various risk factors, including either direct or indirect lung injury, and systemic inflammation triggered also by severe pneumonia (SP). SP-ARDS-associated morbidity and mortality remains high also due to the lack of disease-specific biomarkers. The present study aimed at identifying disease-specific biomarkers in SP or SP-ARDS by integrating proteomic profiles of inflammatory mediators with clinical informatics. Plasma was sampled from the healthy as controls or patients with SP infected with bacteria or infection-associated SP-ARDS on the day of admission, day 3, and day 7. About 15 or 52 cytokines showed significant difference between SP and SP-ARDS patients with controls or 13 between SP-ARDS with SP alone and controls, including bone morphogenetic protein-15 (BMP-15), chemokine (C-X-C motif) ligand 16 (CXCL16), chemokine (C-X-C motif) receptor 3 (CXCR3), interleukin-6 (IL-6), protein NOV homolog (NOV/CCN3), glypican 3, insulin-like growth factor binding protein 4 (IGFBP-4), IL-5, IL-5 R alpha, IL-22 BP, leptin, MIP-1d, and orexin B with a significant correlation with Digital Evaluation Score System (DESS) scores. ARDS patients with overexpressed IL-6, CXCL16, or IGFBP-4 had significantly longer hospital stay and higher incidence of secondary infection. We also found higher levels of those mediators were associated with poor survival rates in patients with lung cancer and involved in the process of the epithelial mesenchymal transition of alveolar epithelial cells. Our preliminary study suggested that integration of proteomic profiles with clinical informatics as part of clinical bioinformatics is important to validate and optimize disease-specific and disease-staged biomarkers.
Keywords: ARDS; Biomarkers; Clinical informatics; Pneumonia; Proteomics.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
