

A retrospective analysis of patient-specific factors on voriconazole clearance
- PMID: 27096102
- PMCID: PMC4835838
- DOI: 10.1186/s40780-016-0044-9
A retrospective analysis of patient-specific factors on voriconazole clearance
Abstract
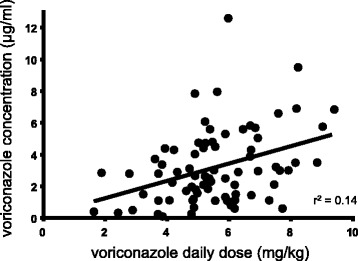
Background: Voriconazole concentrations display a large variability, which cannot completely be explained by known factors. We investigated the relationships of voriconazole concentration with patient-specific variables and concomitant medication to identify clinical factors affecting voriconazole clearance.
Methods: A retrospective chart review of voriconazole trough concentration, laboratory data, and concomitant medication in patients was performed. The concentration/dose ratio (C/D-ratio) was assessed as a surrogate marker of total clearance by dividing voriconazole concentration by daily dose per kg of body weight.
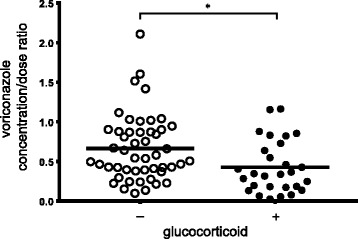
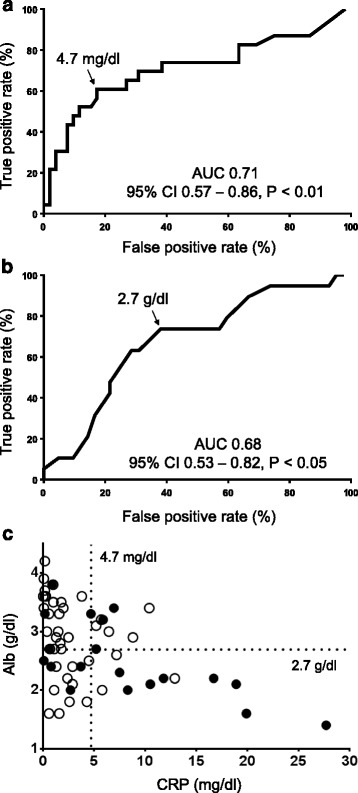
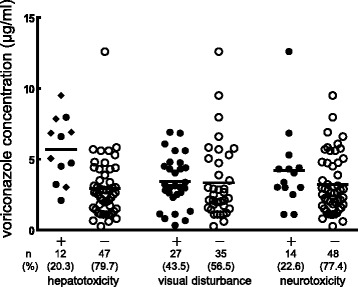
Results: A total of 77 samples from 63 patients were obtained. In multiple linear regression analysis, increased C-reactive protein (CRP) level (p < 0.05) and decreased albumin (Alb) level (p < 0.05) were associated with significantly increased C/D-ratio of voriconazole, and coadministration with a glucocorticoid was associated with significantly (p < 0.05) decreased C/D-ratio of voriconazole (adjusted r (2) = 0.31). Regarding CRP and Alb, receiver operating characteristic curve analysis indicated that increased CRP level and decreased Alb level were significant predictors of toxic trough concentration of voriconazole. For CRP, area under the curve (AUC) and cutoff value were 0.71 (95 % confidence interval (CI), 0.57-0.86, p < 0.01) and 4.7 mg/dl, respectively. For Alb, AUC and cutoff value were 0.68 (95 % CI, 0.53-0.82, p < 0.05) and 2.7 g/dl, respectively. A significant difference was seen in voriconazole trough concentration between patients with hepatotoxicity and those without (5.69 μg/ml vs 3.0 μg/ml, p < 0.001).
Conclusion: Coadministration of glucocorticoid and inflammation, reflected by elevated CRP level and hypoalbuminemia, are associated with voriconazole clearance. We propose that early measurement of voriconazole concentration before the plateau phase will lead to avoidance of a toxic voriconazole level in patients with elevated CRP level and hypoalbuminemia, although further studies are needed to confirm our findings.
Keywords: Drug interaction; Inflammation; Pharmacokinetics; Therapeutic drug monitoring; Voriconazole.
Figures
Similar articles
-
Inflammation is associated with voriconazole trough concentrations.Antimicrob Agents Chemother. 2014 Dec;58(12):7098-101. doi: 10.1128/AAC.03820-14. Epub 2014 Sep 15. Antimicrob Agents Chemother. 2014. PMID: 25223994 Free PMC article.
-
Impact of Inflammation on Voriconazole Exposure in Critically ill Patients Affected by Probable COVID-19-Associated Pulmonary Aspergillosis.Antibiotics (Basel). 2023 Apr 16;12(4):764. doi: 10.3390/antibiotics12040764. Antibiotics (Basel). 2023. PMID: 37107125 Free PMC article.
-
Therapeutic drug monitoring and safety of voriconazole in elderly patients.Int Immunopharmacol. 2020 Jan;78:106078. doi: 10.1016/j.intimp.2019.106078. Epub 2019 Dec 9. Int Immunopharmacol. 2020. PMID: 31830620
-
Combined impact of hypoalbuminemia and pharmacogenomic variants on voriconazole trough concentration: data from a real-life clinical setting in the Chinese population.J Chemother. 2024 May;36(3):179-189. doi: 10.1080/1120009X.2023.2247208. Epub 2023 Aug 20. J Chemother. 2024. PMID: 37599449
-
Mycophenolate, clinical pharmacokinetics, formulations, and methods for assessing drug exposure.Transplant Rev (Orlando). 2011 Apr;25(2):47-57. doi: 10.1016/j.trre.2010.06.001. Epub 2010 Dec 28. Transplant Rev (Orlando). 2011. PMID: 21190834
Cited by
-
Association of procalcitonin with voriconazole concentrations: a retrospective cohort study.BMC Infect Dis. 2024 Sep 10;24(1):952. doi: 10.1186/s12879-024-09862-4. BMC Infect Dis. 2024. PMID: 39256640 Free PMC article.
-
Voriconazole Pharmacokinetics in Critically Ill Patients and Extracorporeal Membrane Oxygenation Support: A Retrospective Comparative Case-Control Study.Antibiotics (Basel). 2023 Jun 25;12(7):1100. doi: 10.3390/antibiotics12071100. Antibiotics (Basel). 2023. PMID: 37508196 Free PMC article.
-
The impact of gene polymorphism and hepatic insufficiency on voriconazole dose adjustment in invasive fungal infection individuals.Front Genet. 2023 Aug 24;14:1242711. doi: 10.3389/fgene.2023.1242711. eCollection 2023. Front Genet. 2023. PMID: 37693307 Free PMC article. Review.
-
Impact of Albumin and Omeprazole on Steady-State Population Pharmacokinetics of Voriconazole and Development of a Voriconazole Dosing Optimization Model in Thai Patients with Hematologic Diseases.Antibiotics (Basel). 2020 Sep 3;9(9):574. doi: 10.3390/antibiotics9090574. Antibiotics (Basel). 2020. PMID: 32899425 Free PMC article.
-
A Large Sample Retrospective Study on the Distinction of Voriconazole Concentration in Asian Patients from Different Clinical Departments.Pharmaceuticals (Basel). 2021 Nov 29;14(12):1239. doi: 10.3390/ph14121239. Pharmaceuticals (Basel). 2021. PMID: 34959640 Free PMC article.
References
-
- Hamada Y, Tokimatsu I, Mikamo H, Kimura M, Seki M, Takakura S, Ohmagari N, Takahashi Y, Kasahara K, Matsumoto K, et al. Practice guidelines for therapeutic drug monitoring of voriconazole: a consensus review of the Japanese Society of Chemotherapy and the Japanese Society of Therapeutic Drug Monitoring. J Infect Chemother. 2013;19:381–392. doi: 10.1007/s10156-013-0607-8. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
