

Identifying immune mechanisms mediating the hypertension during preeclampsia
- PMID: 27097659
- PMCID: PMC4967235
- DOI: 10.1152/ajpregu.00052.2016
Identifying immune mechanisms mediating the hypertension during preeclampsia
Abstract
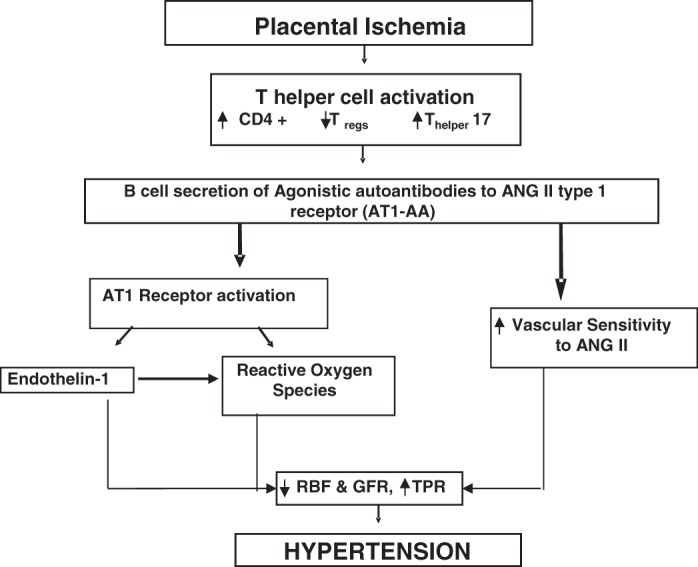
Preeclampsia (PE) is a pregnancy-associated disorder that affects 5-8% of pregnancies and is a major cause of maternal, fetal, and neonatal morbidity and mortality. Hallmark characteristics of PE are new onset hypertension after 20 wk gestation with or without proteinuria, chronic immune activation, fetal growth restriction, and maternal endothelial dysfunction. However, the pathophysiological mechanisms that lead to the development of PE are poorly understood. Recent data from studies of both clinical and animal models demonstrate an imbalance in the subpopulations of CD4+ T cells and a role for these cells as mediators of inflammation and hypertension during pregnancy. Specifically, it has been proposed that the imbalance between two CD4+ T cell subtypes, regulatory T cells (Tregs) and T-helper 17 cells (Th17s), is involved in the pathophysiology of PE. Studies from our laboratory highlighting how this imbalance contributes to vasoactive factors, endothelial dysfunction, and hypertension during pregnancy will be discussed in this review. Therefore, the purpose of this review is to highlight hypertensive mechanisms stimulated by inflammatory factors in response to placental ischemia, thereby elucidating a role.
Keywords: cytokines; hypertension; inflammation; pregnancy.
Copyright © 2016 the American Physiological Society.
Figures
References
-
- AbdAlla S, Lother H, el Massiery A, Quitterer U. Increased AT(1) receptor heterodimers in preeclampsia mediate enhanced angiotensin II responsiveness. Nat Med 7: 1003–1009, 2001. - PubMed
-
- Amaral LM, Kiprono L, Cornelius DC, Shoemaker C, Wallace K, Moseley J, Wallukat G, Martin JN Jr, Dechend R, LaMarca B. Progesterone supplementation attenuates hypertension and the autoantibody to the angiotensin II type I receptor in response to elevated interleukin-6 during pregnancy. Am J Obstet Gynecol 211: 158.e1–158.e6, 2014. - PMC - PubMed
-
- András IE, Pu H, Deli MA, Nath A, Hennig B, Toborek M. HIV-1 Tat protein alters tight junction protein expression and distribution in cultured brain endothelial cells. J Neurosci Res 74: 255–265, 2003. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials