

Parent Use and Efficacy of a Self-Administered, Tablet-Based Parent Training Intervention: A Randomized Controlled Trial
- PMID: 27098111
- PMCID: PMC4867750
- DOI: 10.2196/mhealth.5202
Parent Use and Efficacy of a Self-Administered, Tablet-Based Parent Training Intervention: A Randomized Controlled Trial
Abstract
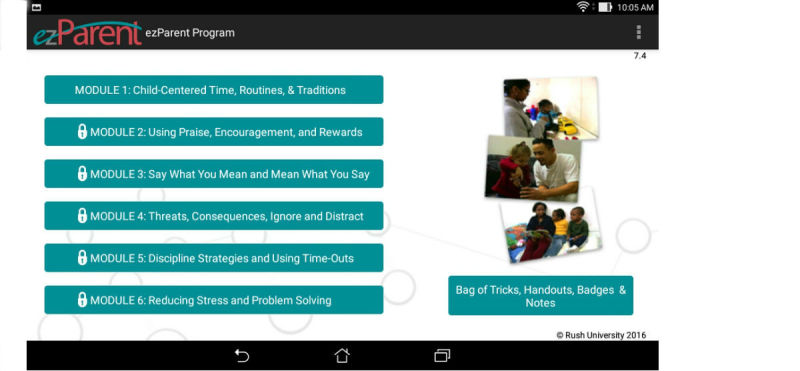
Background: Parent training programs are traditionally delivered in face-to-face formats and require trained facilitators and weekly parent attendance. Implementing face-to-face sessions is challenging in busy primary care settings and many barriers exist for parents to attend these sessions. Tablet-based delivery of parent training offers an alternative to face-to-face delivery to make parent training programs easier to deliver in primary care settings and more convenient and accessible to parents. We adapted the group-based Chicago Parent Program (CPP) to be delivered as a self-administered, tablet-based program called the ezParent program.
Objective: The purpose of this study was to (1) assess the feasibility of the ezParent program by examining parent satisfaction with the program and the percent of modules completed, (2) test the efficacy of the ezParent program by examining the effects compared with a control condition for improving parenting and child behavior in a sample of low-income ethnic minority parents of young children recruited from a primary care setting, and (3) compare program completion and efficacy with prior studies of the group-based CPP.
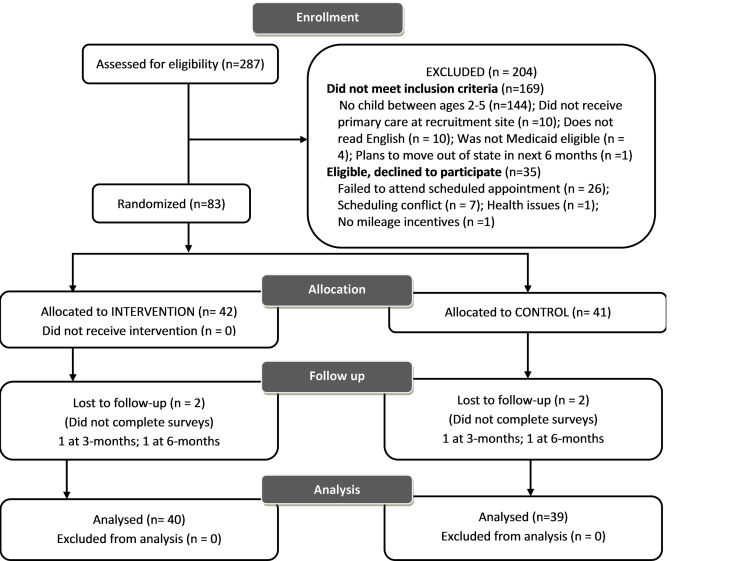
Methods: The study used a two-group randomized controlled trial (RCT) design with repeated measures follow up. Subjects (n=79) were randomly assigned to an intervention or attention control condition. Data collection was at baseline and 12 and 24 weeks post baseline. Parents were recruited from a large, urban, primary care pediatric clinic. ezParent module completion was calculated as the percentage of the six modules completed by the intervention group parents. Attendance in the group-based CPP was calculated as the percentage of attendance at sessions 1 through 10. Satisfaction data were summarized using item frequencies. Parent and child data were analyzed using a repeated measures analysis of variance (RM-ANOVA) with simple contrasts to determine if there were significant intervention effects on the outcome measures. Effect sizes for between group comparisons were calculated for all outcome variables and compared with CPP group based archival data.
Results: ezParent module completion rate was 85.4% (34.2/40; 95% confidence interval [CI] = 78.4%-93.7%) and was significantly greater (P<.05) than face-to-face CPP group attendance (135.2/267, 50.6%) attendance of sessions; 95% CI = 46.8%-55.6%). ezParent participants reported the program as very helpful (35/40, 88.0%) and they would highly recommend the program (33/40, 82.1%) to another parent. ezParent participants showed greater improvements in parenting warmth (F1,77 = 4.82, P<.05) from time 1 to 3. No other significant differences were found. Cohen's d effect sizes for intervention group improvements in parenting warmth, use of corporal punishment, follow through, parenting stress, and intensity of child behavior problems were comparable or greater than those of the group-based CPP.
Conclusions: Data from this study indicate the feasibility and acceptability of the ezParent program in a low-income, ethnic minority population of parents and comparable effect sizes with face-to-face delivery for parents.
Keywords: Internet, intervention, mobile app, mobile health, parenting, prevention.
Conflict of interest statement
Conflicts of Interest: Under an agreement between Rush University Medical Center and Dr. Deborah Gross. Dr. Gross is entitled to revenue from sales of the Chicago Parent Program and the adaptation described in this article. This arrangement has been reviewed and approved by the Johns Hopkins University in accordance with its conflict of interest policies.
Figures
Similar articles
-
Implementation of a Parent Training Program During Community-Based Dissemination (From In-Person to Hybrid): Mixed Methods Evaluation.JMIR Pediatr Parent. 2024 Jul 3;7:e55280. doi: 10.2196/55280. JMIR Pediatr Parent. 2024. PMID: 38959504 Free PMC article.
-
A Randomized Trial of Digitally Delivered, Self-Administered Parent Training in Primary Care: Effects on Parenting and Child Behavior.J Pediatr. 2021 Apr;231:207-214.e4. doi: 10.1016/j.jpeds.2020.12.016. Epub 2020 Dec 16. J Pediatr. 2021. PMID: 33338496 Free PMC article. Clinical Trial.
-
A study protocol testing the implementation, efficacy, and cost effectiveness of the ezParent program in pediatric primary care.Contemp Clin Trials. 2016 Sep;50:229-37. doi: 10.1016/j.cct.2016.08.017. Epub 2016 Aug 31. Contemp Clin Trials. 2016. PMID: 27592122 Free PMC article. Clinical Trial.
-
A Literature Review of Digital Behavioral Parent Training Programs for Parents of Adolescents.Prev Sci. 2024 Jan;25(1):155-174. doi: 10.1007/s11121-023-01596-0. Epub 2023 Oct 16. Prev Sci. 2024. PMID: 37843761 Free PMC article. Review.
-
Helping Latino Parents Learn Skills to Manage Their Children's Mental Health Care [Internet].Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2018 Aug. Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2018 Aug. PMID: 37053364 Free Books & Documents. Review.
Cited by
-
The Use of Noncommercial Parent-Focused mHealth Interventions for Behavioral Problems in Youth: Systematic Review.JMIR Mhealth Uhealth. 2024 Sep 24;12:e51273. doi: 10.2196/51273. JMIR Mhealth Uhealth. 2024. PMID: 39316435 Free PMC article.
-
Administrative Dashboard for Monitoring Use of a Web-Based Parent Training Intervention: Usability Study.JMIR Form Res. 2024 Jan 30;8:e53439. doi: 10.2196/53439. JMIR Form Res. 2024. PMID: 38289675 Free PMC article.
-
Child Poverty, Toxic Stress, and Social Determinants of Health: Screening and Care Coordination.Online J Issues Nurs. 2018 Sep;23(3):2. doi: 10.3912/OJIN.Vol23No03Man02. Epub 2018 Sep 30. Online J Issues Nurs. 2018. PMID: 31427855 Free PMC article.
-
Socioeconomic factors and parents' preferences for internet- and mobile-based parenting interventions to prevent youth mental health problems: A discrete choice experiment.Internet Interv. 2022 Mar 8;28:100522. doi: 10.1016/j.invent.2022.100522. eCollection 2022 Apr. Internet Interv. 2022. PMID: 35309756 Free PMC article.
-
The Role of Parent Engagement in a Web-Based Preventive Parenting Intervention for Child Mental Health in Predicting Parenting, Parent and Child Outcomes.Int J Environ Res Public Health. 2022 Feb 15;19(4):2191. doi: 10.3390/ijerph19042191. Int J Environ Res Public Health. 2022. PMID: 35206394 Free PMC article. Clinical Trial.
References
-
- Campbell SB, Spieker S, Burchinal M, Poe MD, NICHD Early Child Care Research Network Trajectories of aggression from toddlerhood to age 9 predict academic and social functioning through age 12. J Child Psychol Psychiatry. 2006;47:791–800. doi: 10.1111/j.1469-7610.2006.01636.x.JCPP1636 - DOI - PubMed
-
- Merikangas KR, He J, Burstein M, Swanson SA, Avenevoli S, Cui L, Benjet C, Georgiades K, Swendsen J. Lifetime prevalence of mental disorders in U.S. adolescents: results from the National Comorbidity Survey Replication--Adolescent Supplement (NCS-A) J Am Acad Child Adolesc Psychiatry. 2010;49:980–989. doi: 10.1016/j.jaac.2010.05.017. http://europepmc.org/abstract/MED/20855043 S0890-8567(10)00476-4 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
