

Maternal vitamin D concentrations during pregnancy, fetal growth patterns, and risks of adverse birth outcomes
- PMID: 27099250
- PMCID: PMC5410992
- DOI: 10.3945/ajcn.115.123752
Maternal vitamin D concentrations during pregnancy, fetal growth patterns, and risks of adverse birth outcomes
Abstract
Background: Maternal vitamin D deficiency during pregnancy may affect fetal outcomes.
Objective: The objective of this study was to examine whether maternal 25-hydroxyvitamin D [25(OH)D] concentrations in pregnancy affect fetal growth patterns and birth outcomes.
Design: This was a population-based prospective cohort in Rotterdam, Netherlands in 7098 mothers and their offspring. We measured 25(OH)D concentrations at a median gestational age of 20.3 wk (range: 18.5-23.3 wk). Vitamin D concentrations were analyzed continuously and in quartiles. Fetal head circumference and body length and weight were estimated by repeated ultrasounds, and preterm birth (gestational age <37 wk) and small size for gestational age (less than the fifth percentile) were determined.
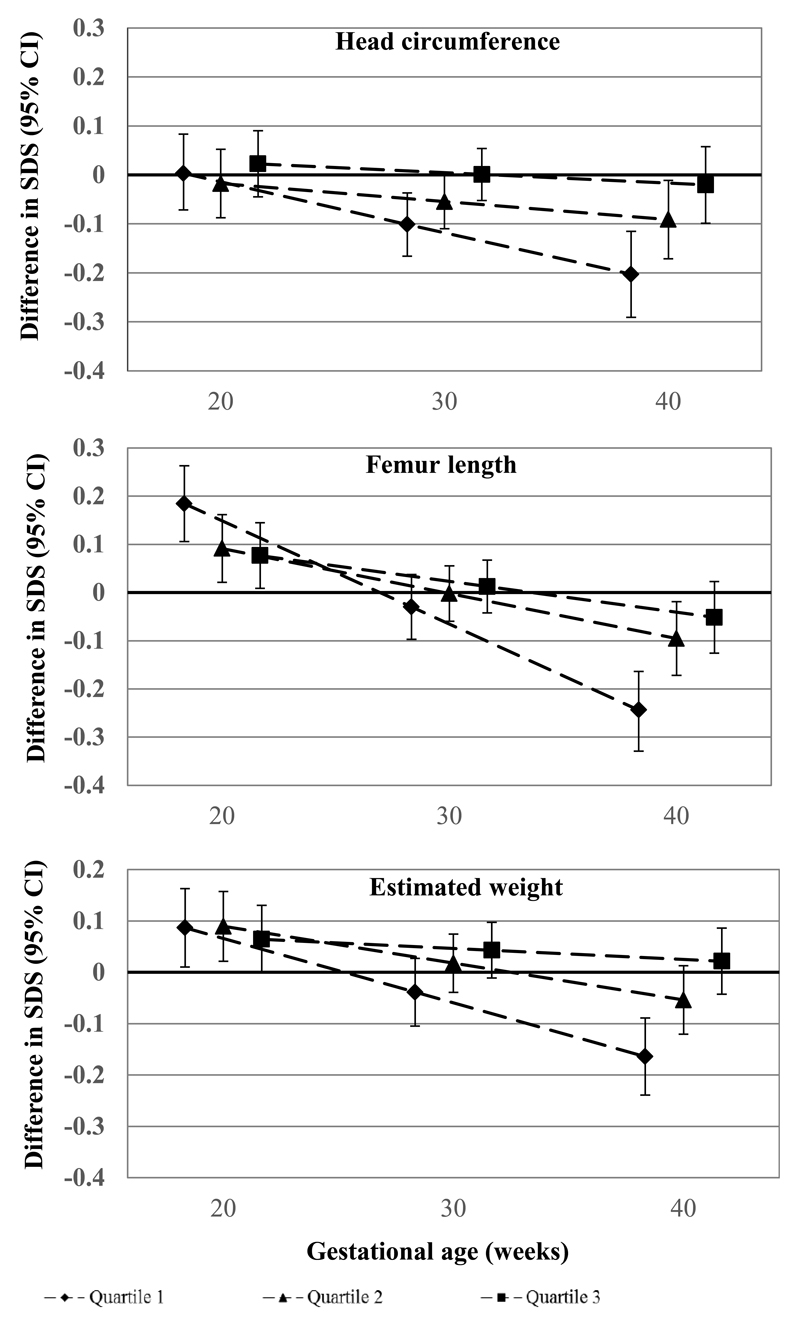
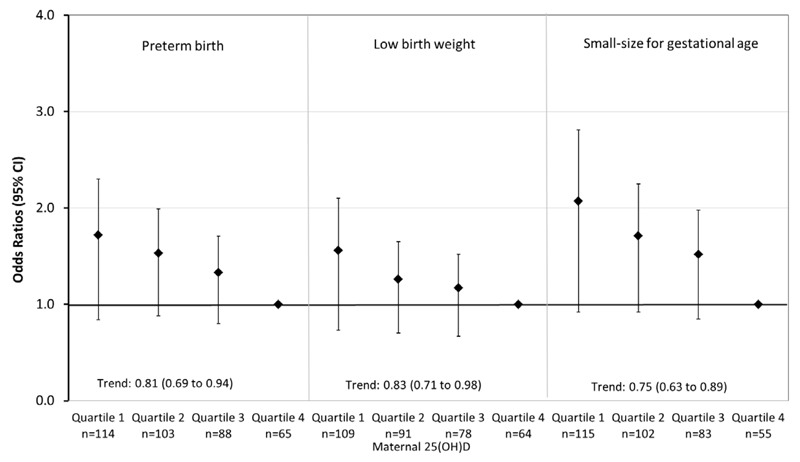
Results: Adjusted multivariate regression analyses showed that, compared with mothers with second-trimester 25(OH)D concentrations in the highest quartile, those with 25(OH)D concentrations in the lower quartiles had offspring with third-trimester fetal growth restriction, leading to a smaller head circumference, shorter body length, and lower body weight at birth (all P < 0.05). Mothers who had 25(OH)D concentrations in the lowest quartile had an increased risk of preterm delivery (OR: 1.72; 95% CI: 1.14, 2.60) and children who were small for gestational age (OR: 2.07; 95% CI: 1.33, 3.22). The estimated population attributable risk of 25(OH)D concentrations <50 nmol/L for preterm birth or small size for gestational age were 17.3% and 22.6%, respectively. The observed associations were not based on extreme 25(OH)D deficiency, but presented within the common ranges.
Conclusions: Low maternal 25(OH)D concentrations are associated with proportional fetal growth restriction and with an increased risk of preterm birth and small size for gestational age at birth. Further studies are needed to investigate the causality of these associations and the potential for public health interventions.
Keywords: 25(OH)D; birth weight; fetal growth; pediatrics; pregnancy; preterm birth; small-size for gestational age; vitamin D.
© 2016 American Society for Nutrition.
Conflict of interest statement
Figures
Similar articles
-
Maternal vitamin D status, fetal growth patterns, and adverse pregnancy outcomes in a multisite prospective pregnancy cohort.Am J Clin Nutr. 2025 Feb;121(2):376-384. doi: 10.1016/j.ajcnut.2024.11.018. Epub 2024 Nov 20. Am J Clin Nutr. 2025. PMID: 39577494 Free PMC article.
-
Umbilical Cord Serum 25-Hydroxyvitamin D Concentrations and Relation to Birthweight, Head Circumference and Infant Length at Age 14 Days.Paediatr Perinat Epidemiol. 2016 May;30(3):238-45. doi: 10.1111/ppe.12288. Epub 2016 Feb 24. Paediatr Perinat Epidemiol. 2016. PMID: 27038010 Free PMC article.
-
Associations of maternal and fetal vitamin D status with childhood body composition and cardiovascular risk factors.Matern Child Nutr. 2019 Apr;15(2):e12672. doi: 10.1111/mcn.12672. Epub 2018 Sep 21. Matern Child Nutr. 2019. PMID: 30238610 Free PMC article.
-
Vitamin D and pregnancy outcomes: Overall results of the FEPED study.J Gynecol Obstet Hum Reprod. 2020 Oct;49(8):101883. doi: 10.1016/j.jogoh.2020.101883. Epub 2020 Jul 27. J Gynecol Obstet Hum Reprod. 2020. PMID: 32730862 Review.
-
Vitamin D Supplementation during Pregnancy: An Evidence Analysis Center Systematic Review and Meta-Analysis.J Acad Nutr Diet. 2020 May;120(5):898-924.e4. doi: 10.1016/j.jand.2019.07.002. Epub 2019 Oct 25. J Acad Nutr Diet. 2020. PMID: 31669079
Cited by
-
Predictive value of Vitamin D levels in pregnant women on gestational length and neonatal weight in China: a population-based retrospective study.Reprod Biol Endocrinol. 2024 Aug 13;22(1):102. doi: 10.1186/s12958-024-01276-w. Reprod Biol Endocrinol. 2024. PMID: 39138489 Free PMC article.
-
Low Dietary Intakes of Essential Nutrients during Pregnancy in Vietnam.Nutrients. 2018 Aug 6;10(8):1025. doi: 10.3390/nu10081025. Nutrients. 2018. PMID: 30082626 Free PMC article.
-
The Associations of Maternal and Neonatal Vitamin D with Dental Development in Childhood.Curr Dev Nutr. 2019 Mar 7;3(4):nzy100. doi: 10.1093/cdn/nzy100. eCollection 2019 Apr. Curr Dev Nutr. 2019. PMID: 30931425 Free PMC article.
-
Relationship between vitamin D status and the vaginal microbiome during pregnancy.J Perinatol. 2019 Jun;39(6):824-836. doi: 10.1038/s41372-019-0343-8. Epub 2019 Mar 11. J Perinatol. 2019. PMID: 30858609 Free PMC article. Clinical Trial.
-
Combined Effect of Maternal Vitamin D Deficiency and Gestational Diabetes Mellitus on Trajectories of Ultrasound-Measured Fetal Growth: A Birth Cohort Study in Beijing, China.J Diabetes Res. 2020 Mar 30;2020:4231892. doi: 10.1155/2020/4231892. eCollection 2020. J Diabetes Res. 2020. PMID: 32337290 Free PMC article.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
