

Hyponatremia and Hepatorenal Syndrome
- PMID: 27099594
- PMCID: PMC4836593
Hyponatremia and Hepatorenal Syndrome
Abstract
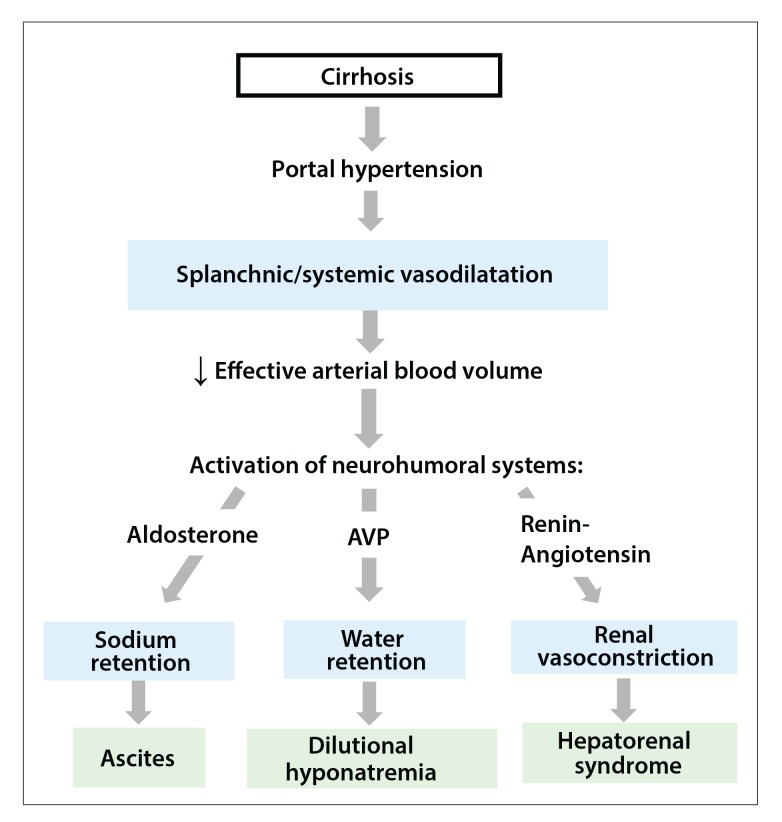
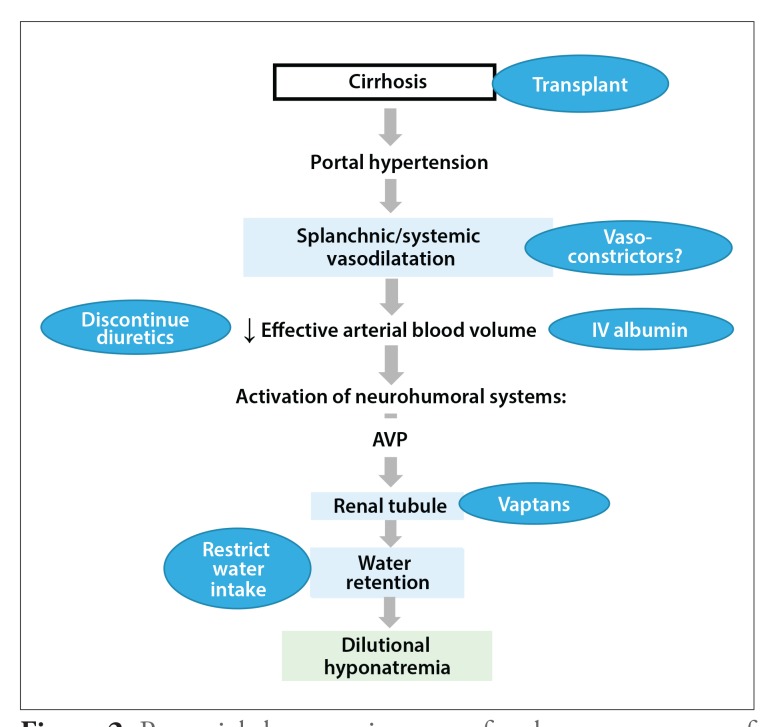
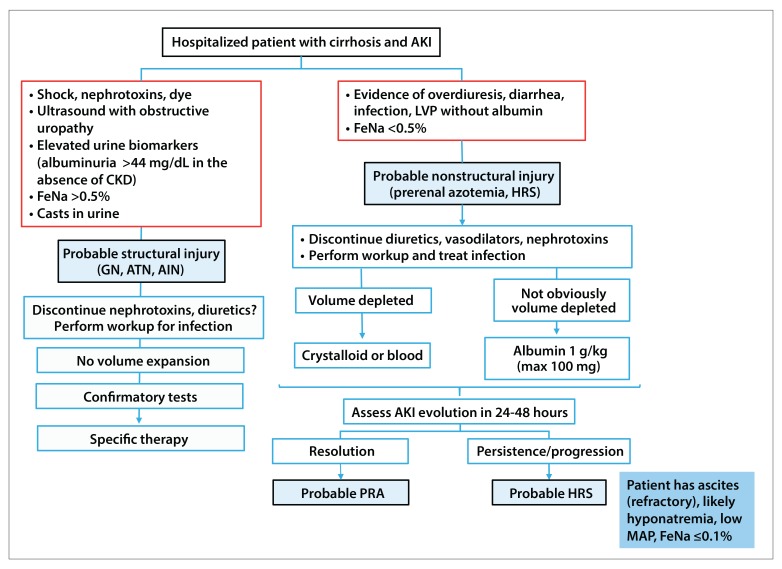
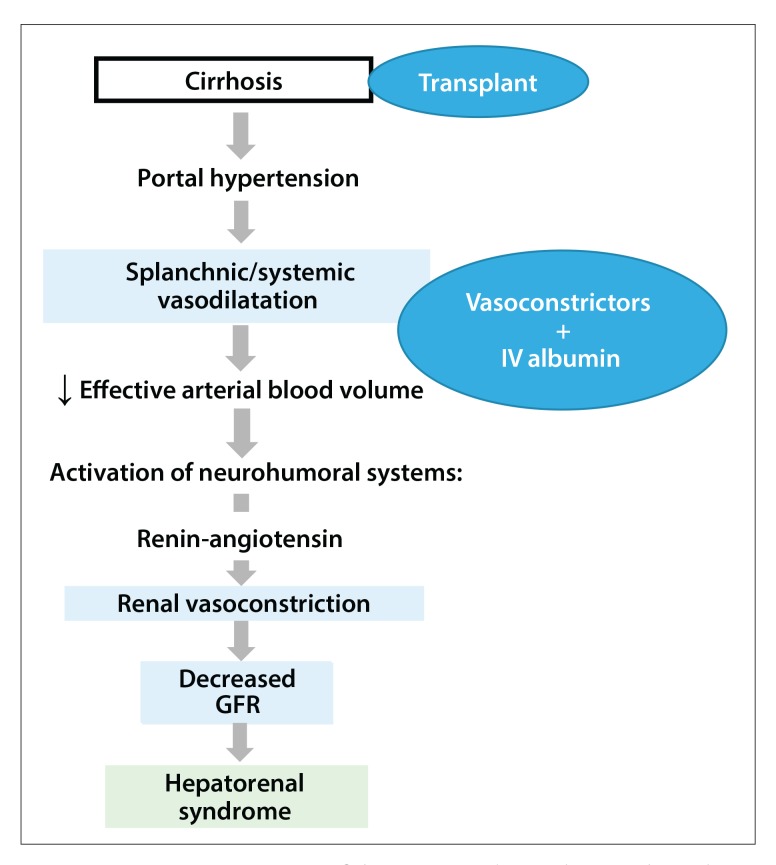
Hyponatremia and hepatorenal syndrome are severe complications in patients with cirrhosis and ascites resulting from circulatory abnormalities (splanchnic and systemic vasodilatation) that develop with portal hypertension. Both conditions are associated with an increased risk of death. Hyponatremia and renal failure may develop in patients with cirrhosis due to causes other than portal hypertension. Making an accurate differential diagnosis is important both therapeutically and prognostically. In this article, we discuss the pathophysiology, diagnosis, differential diagnosis, and management of hyponatremia and hepatorenal syndrome in patients with cirrhosis.
Keywords: Hyponatremia; ascites; cirrhosis; hepatorenal syndrome.
Figures
Similar articles
-
Complications of cirrhosis. II. Renal and circulatory dysfunction. Lights and shadows in an important clinical problem.J Hepatol. 2000;32(1 Suppl):157-70. doi: 10.1016/s0168-8278(00)80423-7. J Hepatol. 2000. PMID: 10728802 Review.
-
Portal hypertension.Curr Opin Gastroenterol. 1999 May;15(3):260-9. doi: 10.1097/00001574-199905000-00012. Curr Opin Gastroenterol. 1999. PMID: 17023954
-
Management of ascites and hepatorenal syndrome.Hepatol Int. 2018 Feb;12(Suppl 1):122-134. doi: 10.1007/s12072-017-9815-0. Epub 2017 Aug 23. Hepatol Int. 2018. PMID: 28836115 Review.
-
Renal dysfunction in patients with chronic liver disease.Electrolyte Blood Press. 2009 Dec;7(2):42-50. doi: 10.5049/EBP.2009.7.2.42. Epub 2009 Dec 31. Electrolyte Blood Press. 2009. PMID: 21468185 Free PMC article.
-
Portal hypertension.Curr Opin Gastroenterol. 2001 May;17(3):281-90. doi: 10.1097/00001574-200105000-00012. Curr Opin Gastroenterol. 2001. PMID: 17031170
Cited by
-
Predictors of Development of Hepatorenal Syndrome in Hospitalized Cirrhotic Patients with Acute Kidney Injury.J Clin Med. 2021 Nov 29;10(23):5621. doi: 10.3390/jcm10235621. J Clin Med. 2021. PMID: 34884323 Free PMC article.
-
Plasma expanders for people with cirrhosis and large ascites treated with abdominal paracentesis.Cochrane Database Syst Rev. 2019 Jun 28;6(6):CD004039. doi: 10.1002/14651858.CD004039.pub2. Cochrane Database Syst Rev. 2019. PMID: 31251387 Free PMC article.
-
Child-Turcotte-Pugh Score, MELD Score and MELD-Na Score as Predictors of Short-Term Mortality among Patients with End-Stage Liver Disease in Northern India.Inflamm Intest Dis. 2020 Feb;5(1):1-10. doi: 10.1159/000503921. Epub 2019 Nov 8. Inflamm Intest Dis. 2020. PMID: 32232049 Free PMC article.
-
COVID-19 and hepatorenal syndrome.World J Gastroenterol. 2022 Oct 21;28(39):5666-5678. doi: 10.3748/wjg.v28.i39.5666. World J Gastroenterol. 2022. PMID: 36338894 Free PMC article. Review.
-
The proportion of Model for End-stage Liver Disease Sodium score attributable to creatinine independently predicts post-transplant survival and renal complications.Clin Transplant. 2020 Mar;34(3):e13817. doi: 10.1111/ctr.13817. Epub 2020 Feb 20. Clin Transplant. 2020. PMID: 32027405 Free PMC article.
References
-
- D’Amico G, Garcia-Tsao G, Pagliaro L. Natural history and prognostic indicators of survival in cirrhosis: a systematic review of 118 studies. J Hepatol. 2006;44(1):217–231. - PubMed
-
- Schrier RW, Arroyo V, Bernardi M, Epstekin M, Henriksen JH, Rodés J. Peripheral arterial vasodilation hypothesis: a proposal for the initiation of renal sodium and water retention in cirrhosis. Hepatology. 1988;8(5):1151–1157. - PubMed
-
- Planas R, Montoliu S, Ballesté B, et al. Natural history of patients hospitalized for management of cirrhotic ascites. Clin Gastroenterol Hepatol. 2006;4(11):1385–1394. - PubMed
-
- Iwakiri Y, Groszmann RJ. The hyperdynamic circulation of chronic liver diseases: from the patient to the molecule. Hepatology. 2006;43(2 suppl 1):S121–S131. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources