

Variability in Motor and Language Recovery during the Acute Stroke Period
- PMID: 27099611
- PMCID: PMC4836126
- DOI: 10.1159/000444149
Variability in Motor and Language Recovery during the Acute Stroke Period
Abstract
Background: Most stroke recovery occurs by 90 days after onset, with proportional recovery models showing an achievement of about 70% of the maximal remaining recovery. Little is known about recovery during the acute stroke period. Moreover, data are described for groups, not for individuals. In this observational cohort study, we describe for the first time the daily changes of acute stroke patients with motor and/or language deficits over the first week after stroke onset.
Methods: Patients were enrolled within 24-72 h after stroke onset with upper extremity hemiparesis, aphasia, or both, and were tested daily until day 7 or discharge with the upper-extremity Fugl-Meyer Assessment of Motor Recovery after Stroke, the Boston Naming Test, and the comprehension domain from the Western Aphasia Battery. Discharge scores, and absolute and proportional changes were examined using t-tests for pairwise comparisons and linear regression to determine relative contributions of initial impairment, lesion volume, and age to recovery over this period.
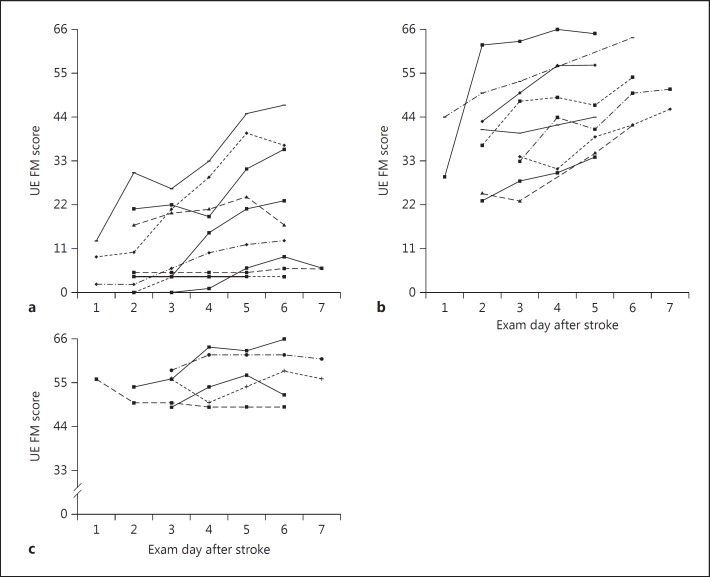
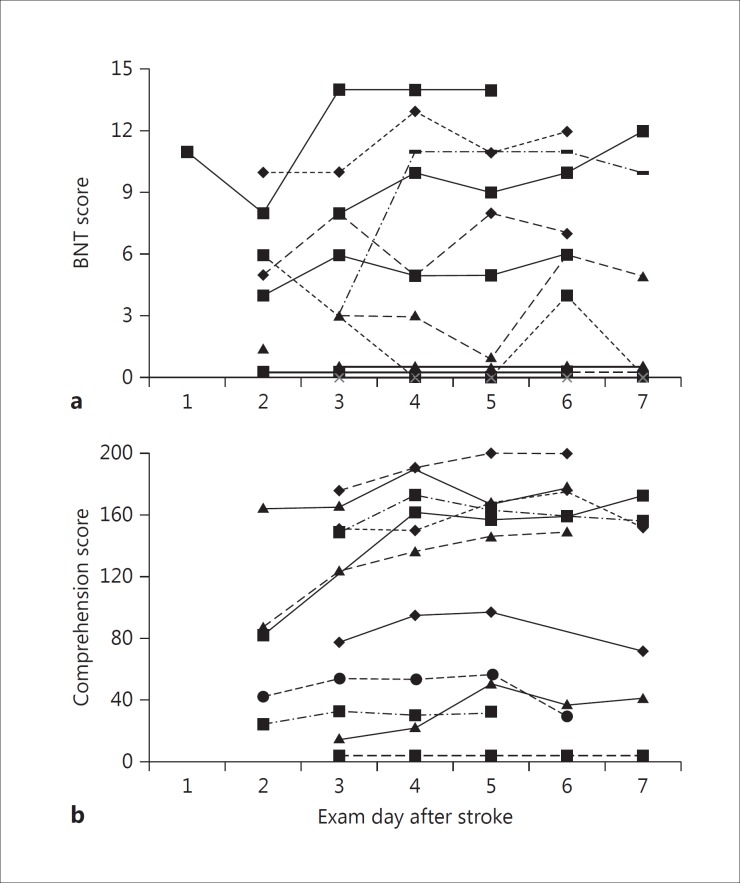
Results: Thirty-four patients were enrolled: 19 had motor deficits alone, 8 had aphasia alone, and 7 had motor and language deficits. In a group analysis, statistically significant changes in absolute scores were found in the motor (p < 0.001) and comprehension (p < 0.001) domains but not in naming. Day-by-day recovery curves for individual patients displayed wide variation with comparable initial impairment. Proportional recovery calculations revealed that, on average, patients achieved less than 1/3 of their potential recovery by the time of discharge. Multivariate regression showed that the amount of variance accounted for by initial severity, age, and lesion volume in this early time period was not significant for motor or language domains.
Conclusions: Over the first week after stroke onset, recovery of upper extremity hemiparesis and aphasia were not predictable on the basis of initial impairment, lesion volume, or age. In addition, patients only achieved about 1/3 of their remaining possible recovery based on the anticipated 70% proportion found at 90 days. These findings suggest that the complex interaction between poststroke structural repair, regeneration, and functional reorganization during the first week after stroke has yet to be elucidated.
Keywords: Acute stroke; Aphasia; Motor impairment; Stroke recovery.
Figures

Similar articles
-
Improvement in aphasia scores after stroke is well predicted by initial severity.Stroke. 2010 Jul;41(7):1485-8. doi: 10.1161/STROKEAHA.109.577338. Epub 2010 Jun 10. Stroke. 2010. PMID: 20538700 Free PMC article.
-
Language changes coincide with motor and fMRI changes following upper extremity motor therapy for hemiparesis: a brief report.Brain Imaging Behav. 2014 Sep;8(3):370-7. doi: 10.1007/s11682-011-9139-y. Brain Imaging Behav. 2014. PMID: 21989635 Clinical Trial.
-
Right hemisphere grey matter structure and language outcomes in chronic left hemisphere stroke.Brain. 2016 Jan;139(Pt 1):227-41. doi: 10.1093/brain/awv323. Epub 2015 Oct 31. Brain. 2016. PMID: 26521078 Free PMC article.
-
Predictors of Poststroke Aphasia Recovery: A Systematic Review-Informed Individual Participant Data Meta-Analysis.Stroke. 2021 May;52(5):1778-1787. doi: 10.1161/STROKEAHA.120.031162. Epub 2021 Mar 15. Stroke. 2021. PMID: 33719515 Free PMC article.
-
Language as a Predictor of Motor Recovery: The Case for a More Global Approach to Stroke Rehabilitation.Neurorehabil Neural Repair. 2019 Mar;33(3):167-178. doi: 10.1177/1545968319829454. Epub 2019 Feb 13. Neurorehabil Neural Repair. 2019. PMID: 30757952 Review.
Cited by
-
Disruptions of resting-state functional connectivity in post-stroke motor dysfunctions: a meta-analysis.Brain Imaging Behav. 2025 Jun;19(3):771-784. doi: 10.1007/s11682-025-00977-z. Epub 2025 Mar 28. Brain Imaging Behav. 2025. PMID: 40148720 Review.
-
Clinical feasibility and cortical effects of synchronous mirror therapy on speech-language and upper limb motor function after stroke.BMC Neurol. 2025 Jul 7;25(1):284. doi: 10.1186/s12883-025-04218-0. BMC Neurol. 2025. PMID: 40624611 Free PMC article.
-
Implementing a Standardized Language Evaluation in the Acute Phases of Aphasia: Linking Evidence-Based Practice and Practice-Based Evidence.Front Neurol. 2020 Jun 1;11:412. doi: 10.3389/fneur.2020.00412. eCollection 2020. Front Neurol. 2020. PMID: 32547472 Free PMC article.
-
Facilitators and barriers to health enhancing physical activity in individuals with severe functional limitations after stroke: A qualitative study.Front Psychol. 2022 Oct 19;13:982302. doi: 10.3389/fpsyg.2022.982302. eCollection 2022. Front Psychol. 2022. PMID: 36337530 Free PMC article.
-
Defining Trajectories of Linguistic, Cognitive-Communicative, and Quality of Life Outcomes in Aphasia: Longitudinal Observational Study Protocol.Arch Rehabil Res Clin Transl. 2024 Apr 2;6(2):100339. doi: 10.1016/j.arrct.2024.100339. eCollection 2024 Jun. Arch Rehabil Res Clin Transl. 2024. PMID: 39006119 Free PMC article.
References
-
- Duncan PW, Goldstein LB, Matchar D, Divine GW, Feussner J. Measurement of motor recovery after stroke. Outcome assessment and sample size requirements. Stroke. 1992;23:1084–1089. - PubMed
-
- Demeurisse G, Demol O, Derouck M, de Beuckelaer R, Coekaerts MJ, Capon A. Quantitative study of the rate of recovery from aphasia due to ischemic stroke. Stroke. 1980;11:455–458. - PubMed
-
- Prabhakaran S, Zarahn E, Riley C, Speizer A, Chong JY, Lazar RM, et al. Inter-individual variability in the capacity for motor recovery after ischemic stroke. Neurorehabil Neural Repair. 2008;22:64–71. - PubMed
-
- Winters C, van Wegen EE, Daffertshofer A, Kwakkel G. Generalizability of the proportional recovery model for the upper extremity after an ischemic stroke. Neurorehabil Neural Repair. 2015;29:614–622. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
