

Predictors of mortality after transjugular portosystemic shunt
- PMID: 27099653
- PMCID: PMC4832094
- DOI: 10.4254/wjh.v8.i11.520
Predictors of mortality after transjugular portosystemic shunt
Abstract
Aim: To investigate if echocardiographic and hemodynamic determinations obtained at the time of transjugular intrahepatic portosystemic shunt (TIPS) can provide prognostic information that will enhance risk stratification of patients.
Methods: We reviewed medical records of 467 patients who underwent TIPS between July 2003 and December 2011 at our institution. We recorded information regarding patient demographics, underlying liver disease, indication for TIPS, baseline laboratory values, hemodynamic determinations at the time of TIPS, and echocardiographic measurements both before and after TIPS. We recorded patient comorbidities that may affect hemodynamic and echocardiographic determinations. We also calculated Model for End-stage Liver Disease (MELD) score and Child Turcotte Pugh (CTP) class. The following pre- and post-TIPS echocardiographic determinations were recorded: Left ventricular ejection fraction, right ventricular (RV) systolic pressure, subjective RV dilation, and subjective RV function. We recorded the following hemodynamic measurements: Right atrial (RA) pressure before and after TIPS, inferior vena cava pressure before and after TIPS, free hepatic vein pressure, portal vein pressure before and after TIPS, and hepatic venous pressure gradient (HVPG).
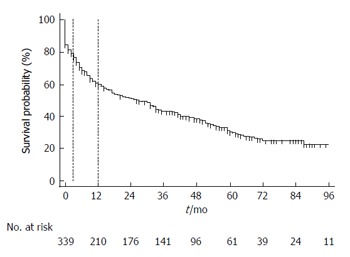
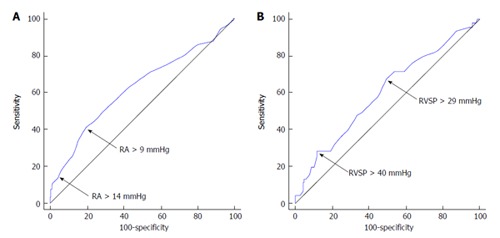
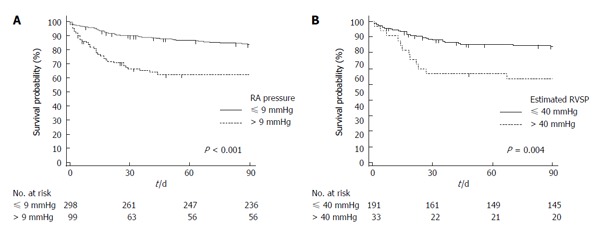
Results: We reviewed 418 patients with portal hypertension undergoing TIPS. RA pressure increased by a mean ± SD of 4.8 ± 3.9 mmHg (P < 0.001), HVPG decreased by 6.8 ± 3.5 mmHg (P < 0.001). In multivariate linear regression analysis, a higher MELD score, lower platelet count, splenectomy and a higher portal vein pressure were independent predictors of higher RA pressure (R = 0.55). Three variables predicted 3-mo mortality after TIPS in a multivariate analysis: Age, MELD score, and CTP grade C. Change in the RA pressure after TIPS predicted long-term mortality (per 1 mmHg change, HR = 1.03, 95%CI: 1.01-1.06, P < 0.012).
Conclusion: RA pressure increased immediately after TIPS particularly in patients with worse liver function, portal hypertension, emergent TIPS placement and history of splenectomy. The increase in RA pressure after TIPS was associated with increased mortality. Age, splenectomy, MELD score and CTP grade were independent predictors of long-term mortality after TIPS.
Keywords: Mortality; Outcomes; Right atrial pressure; Transjugular intrahepatic portosystemic shunt; Transjugular portosystemic shunts.
Figures
References
-
- Rössle M, Haag K, Ochs A, Sellinger M, Nöldge G, Perarnau JM, Berger E, Blum U, Gabelmann A, Hauenstein K. The transjugular intrahepatic portosystemic stent-shunt procedure for variceal bleeding. N Engl J Med. 1994;330:165–171. - PubMed
-
- Ochs A, Rössle M, Haag K, Hauenstein KH, Deibert P, Siegerstetter V, Huonker M, Langer M, Blum HE. The transjugular intrahepatic portosystemic stent-shunt procedure for refractory ascites. N Engl J Med. 1995;332:1192–1197. - PubMed
-
- Gordon FD, Anastopoulos HT, Crenshaw W, Gilchrist B, McEniff N, Falchuk KR, LoCicero J, Lewis WD, Jenkins RL, Trey C. The successful treatment of symptomatic, refractory hepatic hydrothorax with transjugular intrahepatic portosystemic shunt. Hepatology. 1997;25:1366–1369. - PubMed
-
- Malinchoc M, Kamath PS, Gordon FD, Peine CJ, Rank J, ter Borg PC. A model to predict poor survival in patients undergoing transjugular intrahepatic portosystemic shunts. Hepatology. 2000;31:864–871. - PubMed
-
- Garcia-Pagán JC, Heydtmann M, Raffa S, Plessier A, Murad S, Fabris F, Vizzini G, Gonzales Abraldes J, Olliff S, Nicolini A, et al. TIPS for Budd-Chiari syndrome: long-term results and prognostics factors in 124 patients. Gastroenterology. 2008;135:808–815. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
