

Mortality pattern and cause of death in a long-term follow-up of patients with STEMI treated with primary PCI
- PMID: 27099764
- PMCID: PMC4836287
- DOI: 10.1136/openhrt-2016-000405
Mortality pattern and cause of death in a long-term follow-up of patients with STEMI treated with primary PCI
Abstract
Objective: We aimed to assess the pattern of mortality and cause of death in a cohort of patients with ST-segment elevation myocardial infarction (STEMI) treated with primary percutaneous coronary intervention (PCI).
Methods: Consecutive patients with STEMI treated with primary PCI during 2006-2013 were evaluated with a mean follow-up of 3.5 years (1-8.4 years). We used hospital and general practice records and mortality data from The Australian National Death Index.
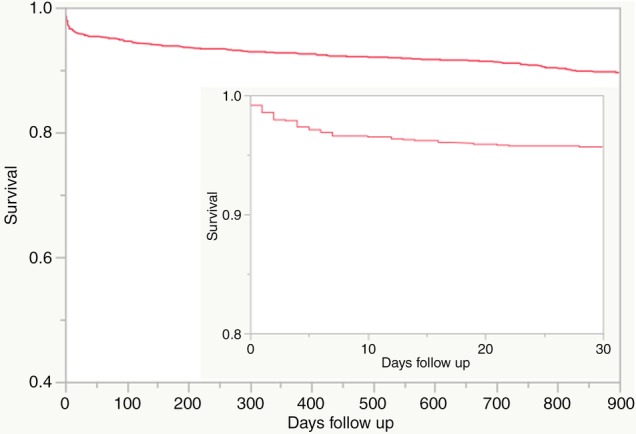
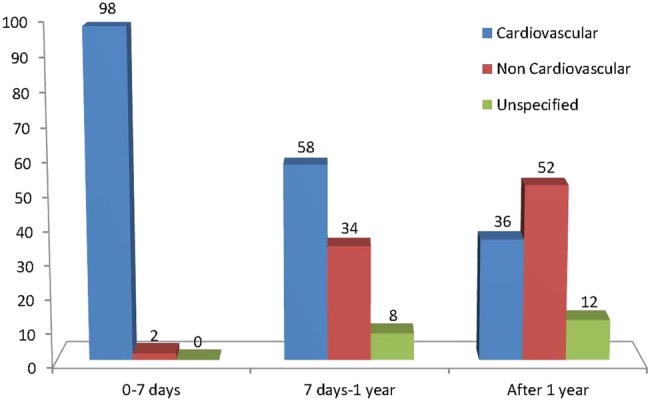
Results: Among 1313 patients (22.5% female) with mean age of 62.3±13.1 years, 181 patients (13.7%) died during long-term follow-up. In the first 7 days, 45 patients (3.4%) died, 76% of these due to cardiogenic shock. Between 7 days and 1 year, another 50 patients died (3.9%), 58% from cardiovascular causes and 22% from cancer. Beyond 1 year, there were 86 deaths with an estimated mean mortality rate of 2.05% per year, 36% of deaths were cardiovascular and 52% non-cardiovascular, including 29% cancer-related deaths. On multivariate analysis, age ≥75 years, history of diabetes, prior PCI, cardiogenic shock, estimated glomerular filtration rate (eGFR) <60 and symptom-to-balloon time >360 min were independent predictors of long-term mortality. In 16 patients who died of sudden cardiac death postdischarge, only 4 (25%) had ejection fraction ≤35% and would have been eligible for an implantable cardioverter defibrillator.
Conclusions: In the era of routine primary PCI, we found a mortality rate of 7.3% at 1 year, and 2.05% per year thereafter. Cause of death was predominantly cardiovascular in the first year and mainly non-cardiovascular after 1 year. Age, diabetes, prior PCI, cardiogenic shock, eGFR <60 and delayed treatment were independent predictors of mortality.
Figures
References
-
- Windecker S, Kolh P, Alfonso F et al. 2014 ESC/EACTS Guidelines on myocardial revascularization. The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J 2014;35:2541–2619. 10.1093/eurheartj/ehu278 - DOI - PubMed
-
- O'Gara PT, Kushner FG, Ascheim DD et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 2013;127:529–55. 10.1161/CIR.0b013e3182742c84 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous