

Effectiveness of four dynamic treatment strategies in patients with anticitrullinated protein antibody-negative rheumatoid arthritis: a randomised trial
- PMID: 27099776
- PMCID: PMC4823586
- DOI: 10.1136/rmdopen-2015-000143
Effectiveness of four dynamic treatment strategies in patients with anticitrullinated protein antibody-negative rheumatoid arthritis: a randomised trial
Abstract
Objective: To determine the most effective treatment strategy among anticitrullinated protein antibodies (ACPA)-negative patients with early rheumatoid arthritis.
Methods: In the BeSt study, 184 ACPA-negative patients were randomised to: (1) sequential monotherapy, (2) step-up therapy, (3) initial combination including prednisone, (4) initial combination including infliximab. Treatment was targeted at the disease activity score (DAS) ≤2.4. Early response and 10-year outcomes were compared between the four strategy-arms in ACPA-negative patients.
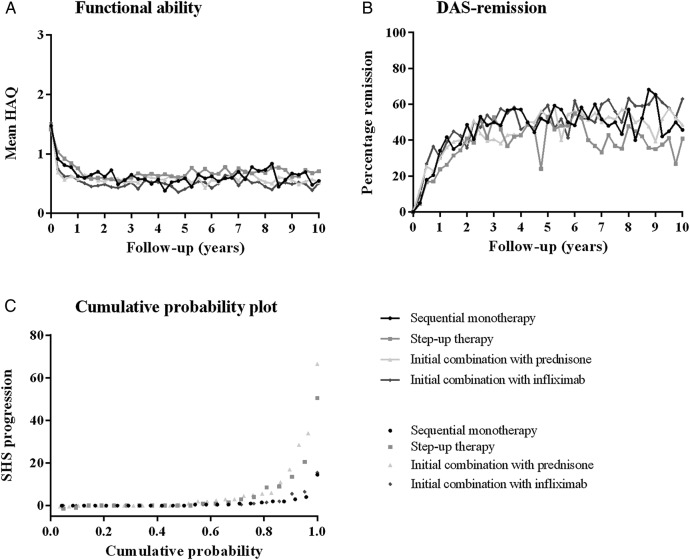
Results: ACPA-negative patients achieved more short-term functional improvement from initial combination therapy than when on monotherapy (at month 3, mean Health Assessment Questionnaire (HAQ) 0.71 vs 0.98, p=0.006; at month 6, 0.59 vs 0.87, p=0.004). Functional ability over time was comparable between the strategy-arms (p=0.551) with a mean HAQ of 0.6 at year 10 (p=0.580 for comparison across the strategy-arms). 10-year radiographic progression was negligible (median 0.5) and comparable between the 4 strategy-arms (p=0.082). At year 10, remission was achieved by 11/40 (28%), 9/45 (20%), 17/56 (30%) and 17/43 patients (40%) in strategy-arms 1-4, respectively (p=0.434). Over time, similar remission percentages were achieved in all strategy-arms (p=0.815). 18%, 16%, 20% and 21% in strategy-arms 1 to 4 (p=0.742) were in drug-free remission at year 10, with a median duration of 60 months across the arms.
Conclusions: Initial combination therapy with methotrexate, sulfasalazine and prednisone, or methotrexate and infliximab, is the most effective treatment strategy for ACPA-negative patients, resulting in earlier functional improvement than when on initial methotrexate monotherapy. After 10 years of targeted treatment, in all strategy-arms favourable clinical outcomes were achieved and radiographic progression was limited.
Trial registration number: NTR262, NTR265.
Keywords: Ant-CCP; Rheumatoid Arthritis; Treatment.
Figures
References
-
- de Vries-Bouwstra JK, Goekoop-Ruiterman YP, Verpoort KN et al. . Progression of joint damage in early rheumatoid arthritis: association with HLA-DRB1, rheumatoid factor, and anti-citrullinated protein antibodies in relation to different treatment strategies. Arthritis Rheum 2008;58:1293–8. 10.1002/art.23439 - DOI - PubMed
-
- Ronnelid J, Wick MC, Lampa J et al. . Longitudinal analysis of citrullinated protein/peptide antibodies (anti-CP) during 5 year follow up in early rheumatoid arthritis: anti-CP status predicts worse disease activity and greater radiological progression. Ann Rheum Dis 2005;64:1744–9. 10.1136/ard.2004.033571 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources