

Development of the A-DIVA Scale: A Clinical Predictive Scale to Identify Difficult Intravenous Access in Adult Patients Based on Clinical Observations
- PMID: 27100437
- PMCID: PMC4845841
- DOI: 10.1097/MD.0000000000003428
Development of the A-DIVA Scale: A Clinical Predictive Scale to Identify Difficult Intravenous Access in Adult Patients Based on Clinical Observations
Abstract
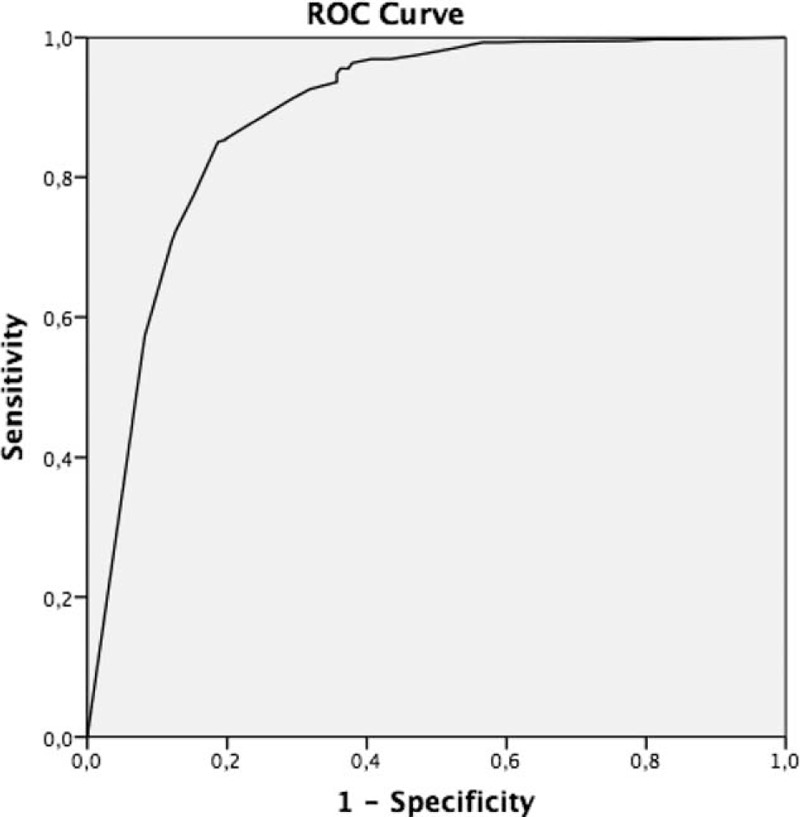
Placement of a peripheral intravenous catheter is a routine procedure in clinical practice, but failure of intravenous cannulation regularly occurs. An accurate and reliable predictive scale for difficult venous access creates the possibility to use other techniques in an earlier time frame. We aimed to develop a predictive scale to identify adult patients with a difficult intravenous access prospectively: the A-DIVA scale. This prospective, observational, cross-sectional cohort study was conducted between January 2014 and January 2015, and performed at the department of anesthesiology of the Catharina Hospital (Eindhoven, The Netherlands). Patients 18 years or older were eligible if scheduled for any surgical procedure, regardless ASA classification, demographics, and medical history. Experienced and certified anesthesiologists and nurse anesthetists routinely obtained peripheral intravenous access. Cannulation was performed regarding standards for care. A failed peripheral intravenous cannulation on the first attempt was the outcome of interest. A population-based sample of 1063 patients was included. Failure of intravenous cannulation was observed in 182/1063 patients (17%). Five variables were associated with a failed first attempt of peripheral intravenous cannulation: palpability of the target vein (OR = 4.94, 95% CI [2.85-8.56]; P < 0.001), visibility of the target vein (OR = 3.63, 95% CI [2.09-6.32]; P < 0.001), a history of difficult peripheral intravenous cannulation (OR = 3.86, 95% CI [2.39-6.25]; P < 0.001), an unplanned indication for surgery (OR = 4.86, 95% CI [2.92-8.07]; P < 0.001), and the vein diameter of at most 2 millimeters (OR = 3.37, 95% CI [2.12-5.36]; P < 0.001). The scoring system was applied in 3 risk groups: 36/788 patients (5%) suffered from a failed first attempt in the low-risk group (A-DIVA score 0 or 1), whereas the medium (A-DIVA score 2 or 3) and high-risk group (A-DIVA score 4 plus), included 72/195 (37%) and 74/80 (93%) patients with a failed first attempt of inserting a peripheral intravenous catheter, respectively. The additive 5-variable A-DIVA scale is a reliable predictive rule that implies the probability to identify patients with a difficult intravenous access prospectively. Dutch Trial Register (ref: 4595).
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
References
-
- Webster J, Osborne S, Rickard CM, et al. Clinically-indicated replacement versus routine replacement of peripheral venous catheters. Cochrane Database Syst Rev 2013; 30:4. - PubMed
-
- Rickard CM, Webster J, Wallis MC, et al. Routine versus clinically indicated replacement of peripheral intravenous catheters: a randomised controlled equivalence trial. Lancet 2012; 380:1066–1074. - PubMed
-
- Aponte H, Acosta S, Rigamonti D, et al. The use of ultrasound for placement of intravenous catheters. AANA J 2007; 75:212–216. - PubMed
-
- Beck RM, Zbierajewski FJ, Barber MK, et al. A comparison of the pain perceived during intravenous catheter insertion after injection with various local anesthetics. AANA J 2011; 79:S58–61. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
