

Long-term outcomes of magnetic resonance imaging-invisible endometrial cancer
- PMID: 27102247
- PMCID: PMC4864514
- DOI: 10.3802/jgo.2016.27.e38
Long-term outcomes of magnetic resonance imaging-invisible endometrial cancer
Abstract
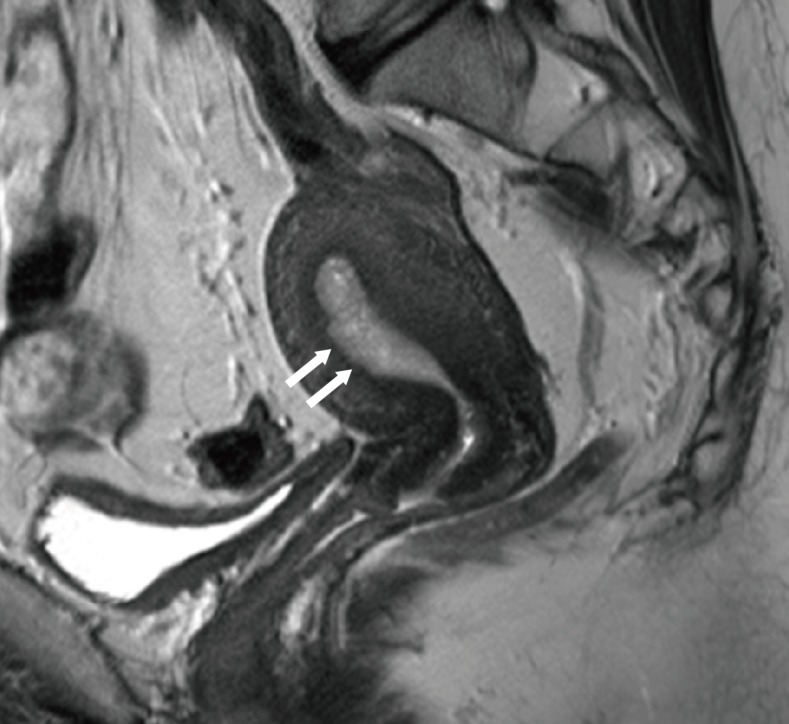
Objective: Magnetic resonance imaging (MRI) is useful for staging endometrial cancer. The treatment and prognosis of MRI-invisible endometrial cancer remain unclear. The purpose of this study was to retrospectively evaluate the long-term outcomes of patients with MRI-invisible endometrial cancer.
Methods: Between February 1995 and December 2011, we reviewed the medical records of 433 patients with endometrial cancer, which was staged IA on MRI. Of these patients, 89 had MRI-invisible cancer and 344 had MRI-visible cancer. Both cancers were treated with simple hysterectomy with or without lymph node dissection according to the surgeon's decision. Both cancers were compared regarding pathologic findings, recurrence rates, and survival rates.
Results: The median sizes of MRI-invisible and MRI-visible cancers were 4 mm (0 to 40 mm) and 20 mm (0 to 89 mm), respectively (p<0.001). Myometrial invasion of these groups were detected in 20.2% (18/89) and 56.7% (195/344), respectively (p<0.001). Lymphadenectomy and follow-up imaging revealed no lymph node metastasis in patients with MRI-invisible cancers, while those revealed in 4.7% (16/344) of patients with MRI-visible cancers (p=0.052). The recurrence rates of MRI-invisible and MRI-visible cancers were 1.1% (1/89) and 7.8% (27/344), respectively (p=0.026). The recurrence-free survival rates of these groups were 98.9% (88/89) and 91.6% (315/344), respectively (p=0.022).
Conclusion: MRI-invisible endometrial cancer can be treated with less invasive surgery because of its lower tumor burden and better prognosis. This cancer may not require lymphadenectomy because of no metastasis or recurrence in lymph nodes.
Keywords: Endometrial Neoplasms; Lymph Nodes; Magnetic Resonance Imaging; Outcome; Stage.
Conflict of interest statement
Figures



Similar articles
-
Postoperative outcomes of MR-invisible stage IB1 cervical cancer.Am J Obstet Gynecol. 2014 Aug;211(2):168.e1-7. doi: 10.1016/j.ajog.2014.02.032. Epub 2014 Mar 4. Am J Obstet Gynecol. 2014. PMID: 24607752
-
Magnetic resonance imaging to identify risk of lymph node metastasis in patients with endometrial cancer.Int J Gynaecol Obstet. 2009 Mar;104(3):233-5. doi: 10.1016/j.ijgo.2008.10.021. Epub 2008 Nov 25. Int J Gynaecol Obstet. 2009. PMID: 19036368
-
Accuracy of preoperative tests in clinical stage I endometrial cancer: the importance of lymphadenectomy.Acta Obstet Gynecol Scand. 2010;89(2):175-81. doi: 10.3109/00016340903418785. Acta Obstet Gynecol Scand. 2010. PMID: 19943822
-
Staging for endometrial cancer: The controversy around lymphadenectomy - Can this be resolved?Best Pract Res Clin Obstet Gynaecol. 2015 Aug;29(6):845-57. doi: 10.1016/j.bpobgyn.2015.02.007. Epub 2015 Mar 4. Best Pract Res Clin Obstet Gynaecol. 2015. PMID: 25817745 Review.
-
Endometrial Cancer and the Role of Lymphadenectomy.Obstet Gynecol Surv. 2016 Jun;71(6):353-60. doi: 10.1097/OGX.0000000000000321. Obstet Gynecol Surv. 2016. PMID: 27302186 Review.
Cited by
-
Using Deep Learning with Convolutional Neural Network Approach to Identify the Invasion Depth of Endometrial Cancer in Myometrium Using MR Images: A Pilot Study.Int J Environ Res Public Health. 2020 Aug 18;17(16):5993. doi: 10.3390/ijerph17165993. Int J Environ Res Public Health. 2020. PMID: 32824765 Free PMC article.
-
Useful MRI Findings for Minimally Invasive Surgery for Early Cervical Cancer.Cancers (Basel). 2021 Aug 13;13(16):4078. doi: 10.3390/cancers13164078. Cancers (Basel). 2021. PMID: 34439231 Free PMC article. Review.
References
-
- Benedetti Panici P, Basile S, Maneschi F, Alberto Lissoni A, Signorelli M, Scambia G, et al. Systematic pelvic lymphadenectomy vs. no lymphadenectomy in early-stage endometrial carcinoma: randomized clinical trial. J Natl Cancer Inst. 2008;100:1707–1716. - PubMed
-
- Todo Y, Kato H, Kaneuchi M, Watari H, Takeda M, Sakuragi N. Survival effect of para-aortic lymphadenectomy in endometrial cancer (SEPAL study): a retrospective cohort analysis. Lancet. 2010;375:1165–1172. - PubMed
-
- Boronow RC, Morrow CP, Creasman WT, Disaia PJ, Silverberg SG, Miller A, et al. Surgical staging in endometrial cancer: clinical-pathologic findings of a prospective study. Obstet Gynecol. 1984;63:825–832. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
