A comparative observational study of inpatient clinical note-entry and reading/retrieval styles adopted by physicians
- PMID: 27103191
- PMCID: PMC5534410
- DOI: 10.1016/j.ijmedinf.2016.02.011
A comparative observational study of inpatient clinical note-entry and reading/retrieval styles adopted by physicians
Abstract
Objective: The objective of this study is to understand physicians' usage of inpatient notes by (i) ascertaining different clinical note-entry and reading/retrieval styles in two different and widely used Electronic Health Record (EHR) systems, (ii) extrapolating potential factors leading to adoption of various note-entry and reading/retrieval styles and (iii) determining the amount of time to task associated with documenting different types of clinical notes.
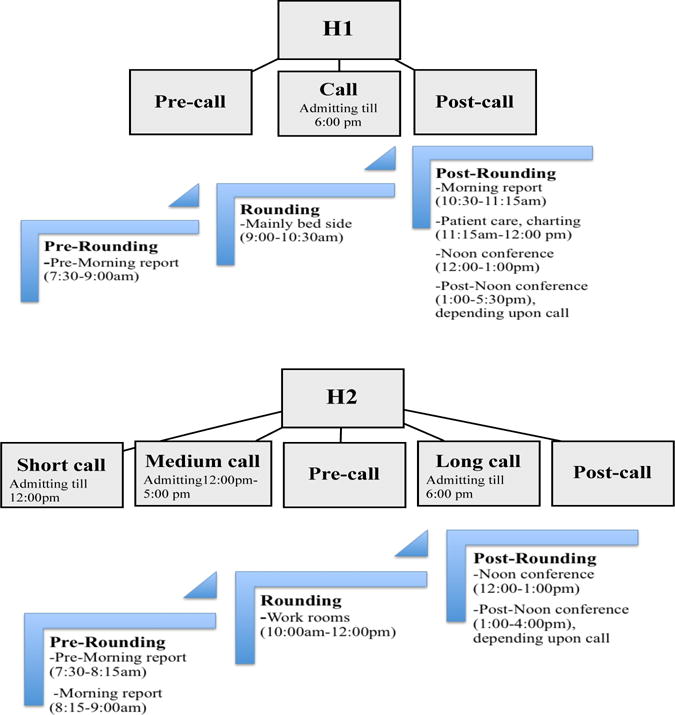
Methods: In order to answer "what" and "why" questions on physicians' adoption of certain-note-entry and reading/retrieval styles, an ethnographic study entailing Internal Medicine residents, with a mixed data analysis approach was performed. Participants were observed interacting with two different EHR systems in inpatient settings. Data was collected around the use and creation of History and Physical (H&P) notes, progress notes and discharge summaries.
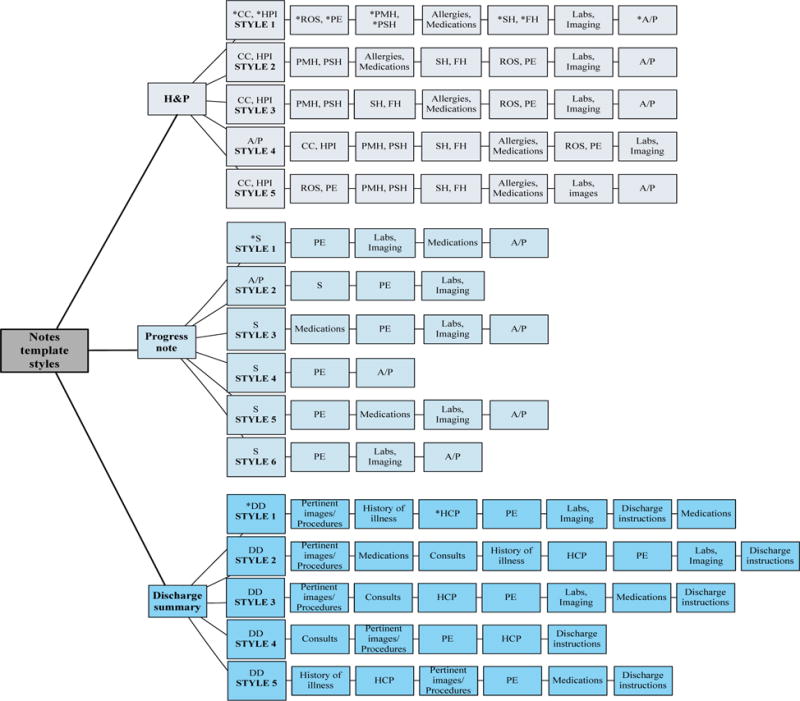
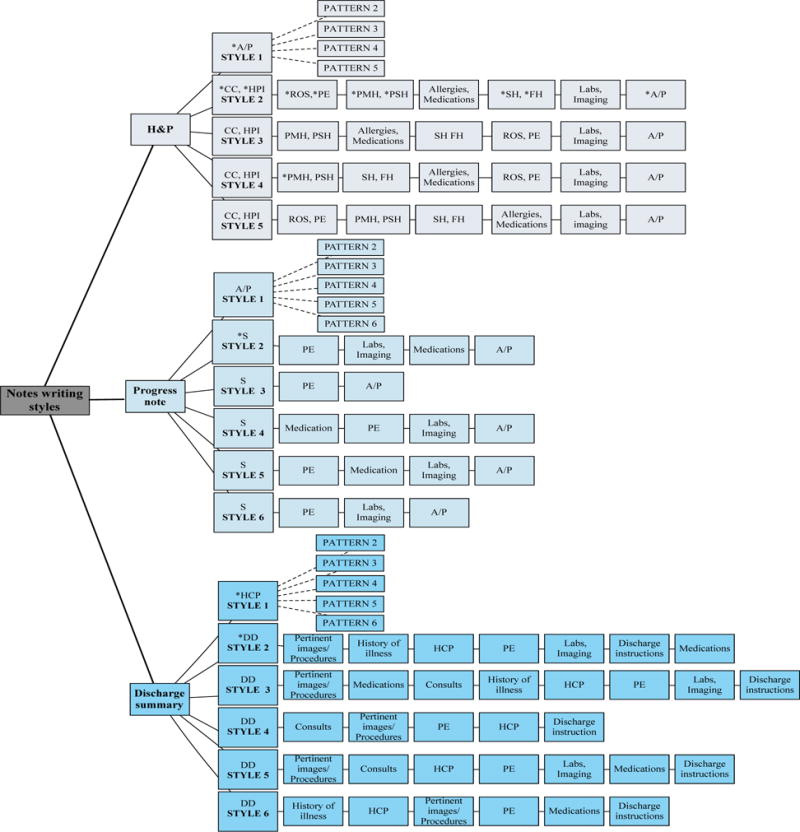
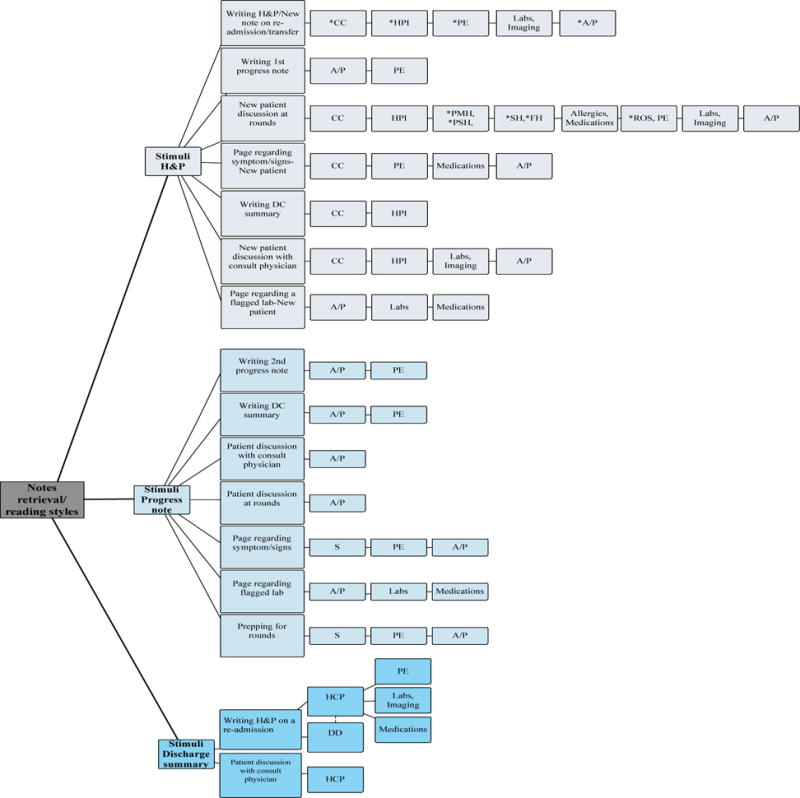
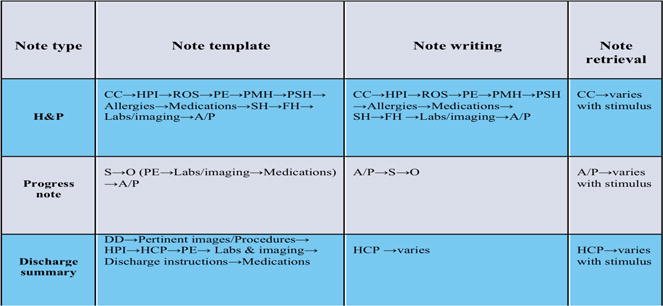
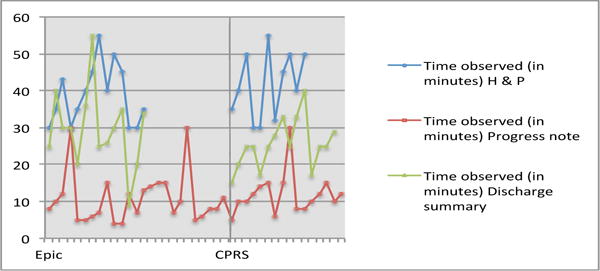
Results: The highest variability in template styles was observed with progress notes and the least variability was within discharge summaries, while note-writing styles were most consistent for H&P notes. The first sections to be read in a H&P and progress note were the Chief Complaint and Assessment & Plan sections, respectively. The greatest note retrieval variability, with respect to the order of how note sections were reviewed, was observed with H&P and progress notes. Physician preference for adopting a certain reading/retrieval order appeared to be a function of what best fits their workflow while fulfilling the stimulus demands. The time spent entering H&P, discharge summaries and progress notes were similar in both EHRs.
Conclusion: This research study unveils existing variability in clinical documentation processes and provides us with important information that could help in designing a next generation EHR Graphical User Interface (GUI) that is more congruent with physicians' mental models, task performance needs, and workflow requirements.
Keywords: Clinical documentation; Electronic health records systems (EHR); Graphical User Interface (GUI); Human-Computer Interaction (HCI); Qualitative analysis; Usability.
Copyright © 2016 Elsevier Ireland Ltd. All rights reserved.
Conflict of interest statement
The authors declare that they have no conflicts of interest in the research.
Figures
References
-
- Solomon DH, Schaffer JL, Katz JN, Horsky J, Burdick E, Nadler E, Bates DW. Can history and physical examination be used as markers of quality?: An analysis of the initial visit note in musculoskeletal care. Med Care [Internet] 2000;38(4):383–91. - PubMed
-
- Weed LL. Medical records, medical education, and patient care: the problem-oriented record as a basic tool. [Internet] Press of Case Western Reserve University; 1970.
-
- Smith K, Smith V, Krugman M, Oman K. Evaluating the impact of computerized clinical documentation. Comput Inform Nurs [Internet] 2005 May-Jun;23(3):132–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials