

Prognostic assessment in COPD without lung function: the B-AE-D indices
- PMID: 27103389
- PMCID: PMC5394475
- DOI: 10.1183/13993003.01485-2015
Prognostic assessment in COPD without lung function: the B-AE-D indices
Abstract
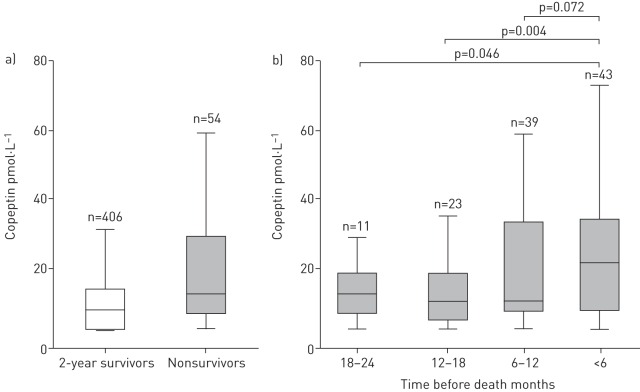
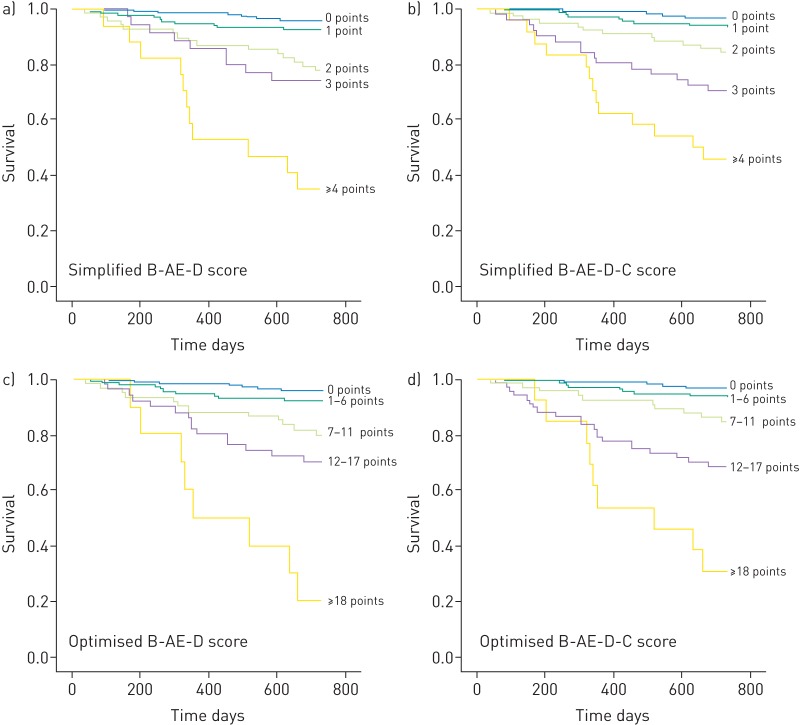
Several composite markers have been proposed for risk assessment in chronic obstructive pulmonary disease (COPD). However, choice of parameters and score complexity restrict clinical applicability. Our aim was to provide and validate a simplified COPD risk index independent of lung function.The PROMISE study (n=530) was used to develop a novel prognostic index. Index performance was assessed regarding 2-year COPD-related mortality and all-cause mortality. External validity was tested in stable and exacerbated COPD patients in the ProCOLD, COCOMICS and COMIC cohorts (total n=2988).Using a mixed clinical and statistical approach, body mass index (B), severe acute exacerbations of COPD frequency (AE), modified Medical Research Council dyspnoea severity (D) and copeptin (C) were identified as the most suitable simplified marker combination. 0, 1 or 2 points were assigned to each parameter and totalled to B-AE-D or B-AE-D-C. It was observed that B-AE-D and B-AE-D-C were at least as good as BODE (body mass index, airflow obstruction, dyspnoea, exercise capacity), ADO (age, dyspnoea, airflow obstruction) and DOSE (dyspnoea, obstruction, smoking, exacerbation) indices for predicting 2-year all-cause mortality (c-statistic: 0.74, 0.77, 0.69, 0.72 and 0.63, respectively; Hosmer-Lemeshow test all p>0.05). Both indices were COPD specific (c-statistic for predicting COPD-related 2-year mortality: 0.87 and 0.89, respectively). External validation of B-AE-D was performed in COCOMICS and COMIC (c-statistic for 1-year all-cause mortality: 0.68 and 0.74; c-statistic for 2-year all-cause mortality: 0.65 and 0.67; Hosmer-Lemeshow test all p>0.05).The B-AE-D index, plus copeptin if available, allows a simple and accurate assessment of COPD-related risk.
Copyright ©ERS 2016.
Conflict of interest statement
Conflict of interest: None declared.
Figures
Comment in
-
Adding biological markers to COPD categorisation schemes: a way towards more personalised care?Eur Respir J. 2016 Jun;47(6):1601-5. doi: 10.1183/13993003.00401-2016. Eur Respir J. 2016. PMID: 27246072 No abstract available.
References
-
- Rosenbaum L, Lamas D. Facing a “slow-motion disaster” – the UN Meeting on noncommunicable diseases. N Engl J Med 2011; 365: 2345–2348. - PubMed
-
- Mannino DM, Buist AS. Global burden of COPD: risk factors, prevalence, and future trends. Lancet 2007; 370: 765–773. - PubMed
-
- Celli BR, Cote CG, Marín JM, et al. . The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med 2004; 350: 1005–1012. - PubMed
-
- Puhan MA, Garcia-Aymerich J, Frey M, et al. . Expansion of the prognostic assessment of patients with chronic obstructive pulmonary disease: the updated BODE index and the ADO index. Lancet 2009; 374: 704–711. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical