

Surgeons' Perspectives on Avoiding Nonbeneficial Treatments in Seriously Ill Older Patients with Surgical Emergencies: A Qualitative Study
- PMID: 27105058
- PMCID: PMC4860675
- DOI: 10.1089/jpm.2015.0450
Surgeons' Perspectives on Avoiding Nonbeneficial Treatments in Seriously Ill Older Patients with Surgical Emergencies: A Qualitative Study
Abstract
Background: Clinical decisions for seriously ill older patients with surgical emergencies are highly complex. Measuring the benefits of burdensome treatments in this context is fraught with uncertainty. Little is known about how surgeons formulate treatment decisions to avoid nonbeneficial surgery, or engage in preoperative conversations about end-of-life (EOL) care.
Objective: We sought to describe how surgeons approach such discussions, and to identify modifiable factors to reduce nonbeneficial surgery near the EOL.
Design: Purposive and snowball sampling were used to recruit a national sample of emergency general surgeons. Semistructured interviews were conducted between February and May 2014.
Measurements: Three independent coders performed qualitative coding using NVivo software (NVivo version 10.0, QSR International). Content analysis was used to identify factors important to surgical decision making and EOL communication.
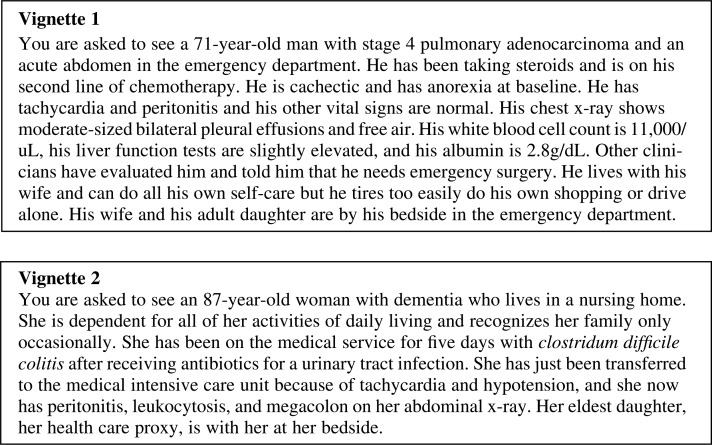
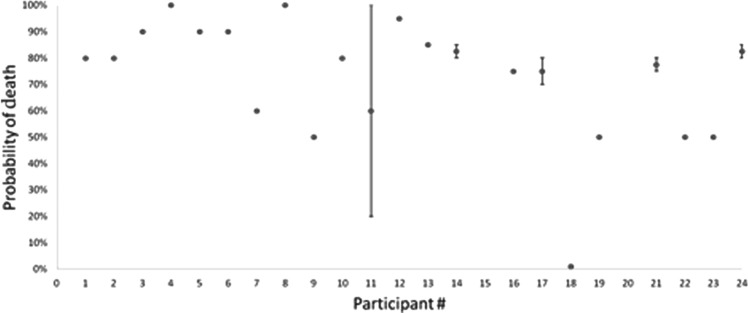
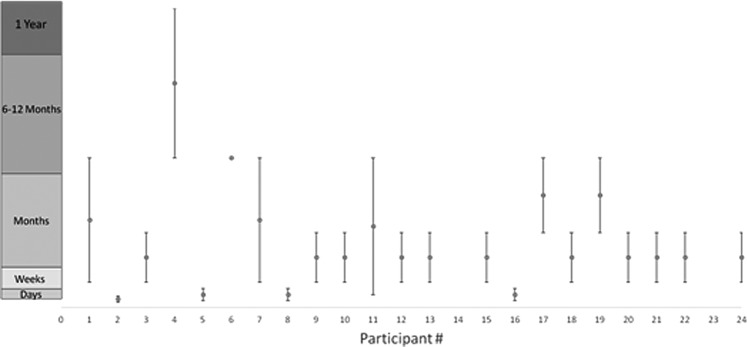
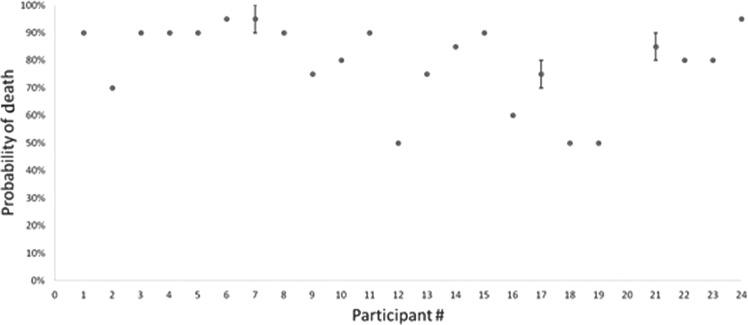
Results: Twenty-four surgeons were interviewed. Participants felt responsible for conducting EOL conversations with seriously ill older patients and their families before surgery to prevent nonbeneficial treatments. However, wide differences in prognostic estimates among surgeons, inadequate data about postoperative quality of life (QOL), patients and surrogates who were unprepared for EOL conversations, variation in perceptions about the role of palliative care, and time constraints are contributors to surgeons providing nonbeneficial operations. Surgeons reported performing operations they knew would not benefit the patient to give the family time to come to terms with the patient's demise.
Conclusions: Emergency general surgeons feel responsible for having preoperative discussions about EOL care with seriously ill older patients to avoid nonbenefical surgery. However, surgeons identified multiple factors that undermine adequate communication and lead to nonbeneficial surgery.
Figures
References
-
- Parekh AK, Barton MB: The challenge of multiple comorbidity for the US health care system. JAMA 2010;303:1303–1304 - PubMed
-
- Cooper Z, Mitchell SL, Gorges RJ, et al. : Predictors of mortality in older patients >30 days after emergent major abdominal operation: Data from the health and retirement survey. J Am Coll Surg 219:S53
-
- Stoneham M, Murray D, Foss N: Emergency surgery: The big three: Abdominal aortic aneurysm, laparotomy and hip fracture. Anaesthesia 2014;69:70–80 - PubMed
-
- Scarborough JE, Pappas TN, Bennett KM, et al. : Failure-to-pursue rescue: Explaining excess mortality in elderly emergency general surgical patients with preexisting “do-not-resuscitate” orders. Ann Surg 2012;256:453–461 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
