

Clinical significance of pneumatosis intestinalis - correlation of MDCT-findings with treatment and outcome
- PMID: 27106233
- PMCID: PMC5127863
- DOI: 10.1007/s00330-016-4348-9
Clinical significance of pneumatosis intestinalis - correlation of MDCT-findings with treatment and outcome
Abstract
Objectives: To evaluate the clinical significance of pneumatosis intestinalis (PI) including the influence on treatment and outcome.
Method and materials: Two radiologists jointly reviewed MDCT-examinations of 149 consecutive emergency patients (53 women, mean age 64, range 21-95) with PI of the stomach (n = 4), small (n = 68) and/or large bowel (n = 96). PI extension, distribution and possibly associated porto-mesenteric venous gas (PMVG) were correlated with other MDCT-findings, risk factors, clinical management, laboratory, histopathology, final diagnosis and outcome.
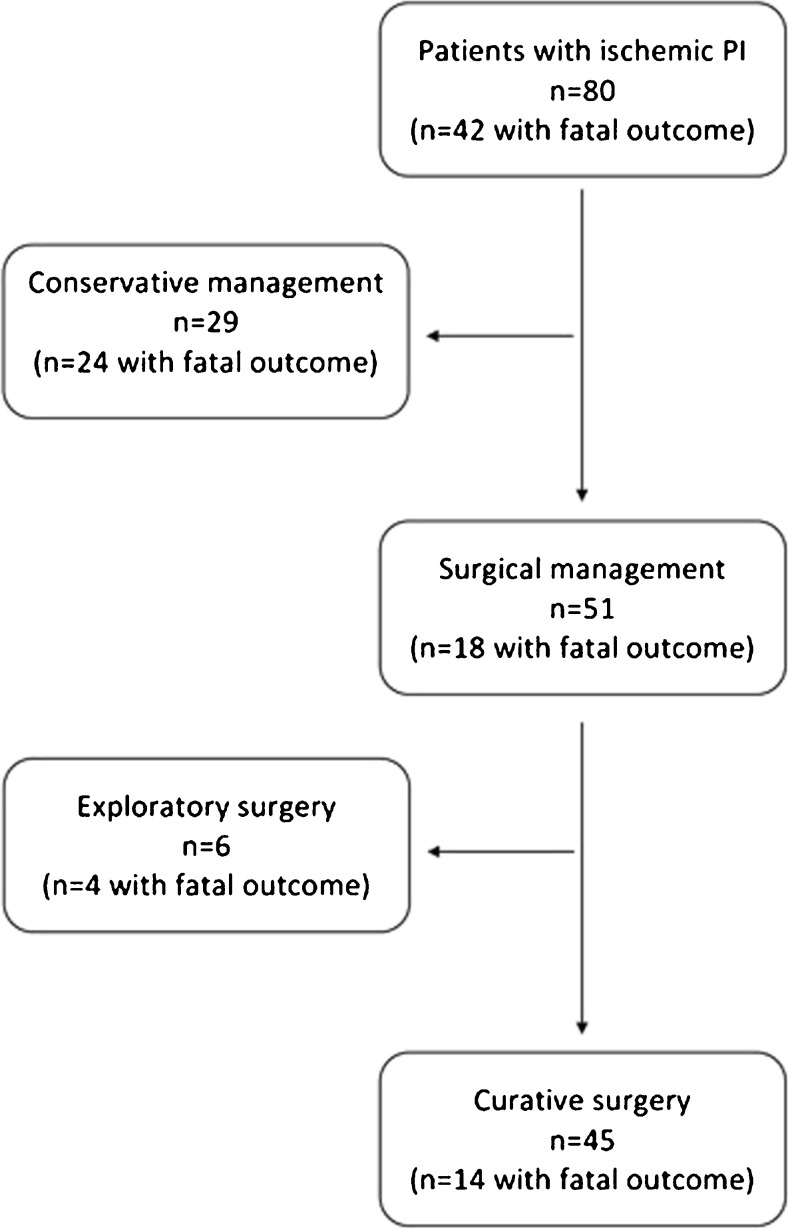
Results: The most frequent cause of PI was intestinal ischemia (n = 80,53.7 %), followed by infection (n = 18,12.1 %), obstructive (n = 12,8.1 %) and non-obstructive (n = 10,6.7 %) bowel dilatation, unknown aetiologies (n = 8,5.4 %), drugs (n = 8,5.4 %), inflammation (n = 7,4.7 %), and others (n = 6,4 %). Neither PI distribution nor extension significantly correlated with underlying ischemia. Overall mortality was 41.6 % (n = 62), mostly related to intestinal ischemia (p = 0.003). Associated PMVG significantly correlated with underlying ischemia (p = 0.009), as did the anatomical distribution of PMVG (p = 0.015). Decreased mural contrast-enhancement was the only other MDCT-feature significantly associated with ischemia (p p < 0.001). Elevated white blood count significantly correlated with ischemia (p = 0.03).
Conclusion: In emergency patients, ischemia remains the most common aetiology of PI, showing the highest mortality. PI with associated PMVG is an alerting sign. PI together with decreased mural contrast-enhancement indicates underlying ischemia.
Key points: • In emergency patients, PI may be caused by various disorders. • Intestinal ischemia remains the most common cause of PI in acute situations. • PI associated with decreased mural contrast-enhancement indicates acute intestinal ischemia. • PI associated with PMVG should alert the radiologist to possible underlying ischemia.
Keywords: Intestinal ischemia; Intestines; Multidetector computed-tomography; Pneumatosis intestinalis; Portomesenteric venous gas.
Figures




References
-
- Du Vernoi JG. Anatomische Beobachtung der unter der äußeren und inneren Haut der Gedärme eingeschlossenen Luft. Phys Med Abhandl Acad Wissensch Petersb. 1783;2:182.
-
- Wolfe JN, Evans WA. Gas in the portal veins of infants: a roentgenographic demonstration with post-mortem anatomical correlation. AJR. 1955;74:486–489. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
